108
TRADITIONAL BIRTH ATTENDANTS A field guide to their training, evaluation, and articulation with health services WORLD HEALTH ORGANIZATION GE~EVA 1979
| Date post: | 22-Feb-2023 |
| Category: |
Documents |
| Upload: | khangminh22 |
| View: | 0 times |
| Download: | 0 times |

TRADITIONAL BIRTH ATTENDANTS
A field guide to their training, evaluation, and articulation with health services
WORLD HEALTH ORGANIZATION GE~EVA
1979

WHO Offset Publication No. 44
PARTICIPANTS IN THE PREPARATION OF THE VOLUME
Beverley Du Gas, formerly Division of Health Manpower Planning, Department of National Health and Welfare, Canada
Amelia Mangay-Maglacas, Senior Scientist for Nursing, Division of Health Manpower Development, WHO
Helena Pizurki, Division of Manpower Development, WHO
John Simons, Centre for Population Studies, London School of Hygiene and Tropical Medicine,. London, England
Review and comment: Alicia Gil del Real, Director of Training, Margaret Sanger Center, New York, USA; and the following WHO staff: Henry Bannerman, Elizabeth Barton, Inge Brilggemann, Karen Edstrom, Fred Katz, Leila Mehra, Dev Ray.
ACKNOWLEDGEMENTS
The World Health Organization is particularly grateful to Beverley Du Gas, formerly of the Division of Health Manpower Planning, Department of Health and National Welfare, Canada, and to John Simons, of the Centre for Population Studies, London School of Hygiene and Tropical Medicine, for their valuable assistance, as Consultants to the Organization, in the development of many aspects of the process described in this publication.
Acknowledgement of indebtedness is also made to the persons whose reports are cited as references and to those who kindly provided useful unpublished material. Their names appear in the final part of this publication.
The planning, preparation, and publication of this guide were made possible by a generous grant from the United Nations Fund for Population Activities.

CONTENTS
Preface
Introduction
1.
2.
3.
4.
5.
6.
7.
Overview of programme planning and development
Formulation of basic policies (ground rules)
Promotion of basic policies
3.1 Promotional campaign addressed to health professionals
3.2 Promotional campaign addressed to TBAs
3.3 Promotional campaign addressed to the community
Information-gathering for programme development
4.1 Information on maternal and child health and family planning services
4.2 Inventory of TBAs
4.3 Information on local beliefs and practices
Planning and development of the training programme
5.1 Definition of functions and tasks of the training programme
5.2 Selection and preparation of trainers
5.3 Selection of trainees
5.4 Development of the course
Evaluation of the training prograrmne
6.1 Evaluation of trainees
6.2 Evaluation of teaching/learning materials and methods
6.3 Evaluation of the trainers
6.4 Evaluation of learning objectives
Articulation of TBA's activities with the organized health system
7.1 Orientation of staff
7.2 Supervision and continuing education of the TBA
7.3 Supporting services
7.4 Records and reports
7.5 Relationship of TBAs to other health workers
7.6 Regulation of the TBA's practice
7.7 Maintenance of interest in the programme
5
7
9
12
13
14
14
15
15
15
16
17
21
21
22
23
24
27
27
28
29
29
29
30
30
32
34
35
36
37

- 4 -
8. Progrannne evaluation
8.1 Assessment of the training programme
8.2 Assessment of the performance of trained
8.3 Assessment of impact on health status
8.4 Conclusions
Figures
Notes and references
TBAs
37
38
38
41
42
45
89

- 5 -
PREFACE
• The present publication constitutes part of a group of publications and documents that the World Health Organization has prepared (or, in some cases, is in the process of preparing) in order to help health administrators, as well as educators, trainers, and supervisors of health workers, to examine, evaluate and, where feasible, strengthen current programmes through which traditional birth attendants (TBAs) are trained and used in the area of maternal and child health and family planning, or to develop new programmes in this regard, if necessary. This publication was preceded by one entitled The traditional birth attend.ant in maternal and child heal th and family planning: a guide to her training and utilization, 1 It is in no way intended to replace its predecessor, which contains a great deal of valuable information and guidelines. In fact, many of the notions contained in that publication are, perforce, reflected here, but in contexts suited to the purpose of the present publication, which is to provide a systematic framework for the planning, implementation, and evaluation of programmes for the training and utilization of TBAs for work in maternal and child.health and family planning. Additionally, the Organization has prepared an annotated bibliography of literature on the training, use, and evaluation of TBAs. Plans are under way for the undertaking of country case studies concerning the training and use of TBAs. The reports of these studies will collectively cover a variety of special themes, e.g., the TBA as a primary health care worker; the development and use of a national registry of TBAs; the use of maternity centres staffed by TBAs as a means of achieving maximum effect with a minimum of supervision; and the role and impact of the TBA in family planning.
• The guidelines presented in this publication were prepared with a view to the develop-ment of nation-wide programmes for the training, utilization, and evaluation of TBAs. In countries where the desire may be to start (or continue) the development of programmes on a more modest scale, e.g., at a provincial, district, or even lower level of community organization, the procedures for planning, implementing, and evaluating the programme concerned would be largely similar to those described herein for a nation-wide programme, The main differences would lie in: (a) the administrative level and nature of the body responsible for making the decision to develop the programme, for defining relevant policies, and for the planning, promotion, implementation, and evaluation of the programme; (b) the sources of financial and other forms of support needed for the programme; and (c) the administrative level up to which the reporting system would reach for purposes of programme evaluation and further planning. It may thus be useful for certain readers to substitute mentally for specified terms such as "central level", "government level", and "national level" terms such as "regional level", "provincial level", and "state level", and, for the latter, terms indicating lower levels of administration, as appropriate.
• While the settings of TBA programmes often have some characteristics in common, they also differ in many important respects. For this reason particularly, it was considered essential to present guidelines that could be applied generally and to illustrate these, as far as was found practicable, with summary descriptions or models of procedures that have actually been used in TBA programmes, An attempt has been made to arrange the content of this publication in a way that will accommodate both individuals whose work requires only a general idea of what i? involved in planning, implementing, and evaluating a
1 See note 1, page 90.

- 6 -
programme for the training and utilization of TBAs and those whose work necessitates as much detailed information as possiole on this subject. Thus, the publication has three distinct parts. The first part (the main body of the text) provides suggestions regarding the basic elements to be considered in the process mentioned above and, at the same time, indicates (throughout the text) the various models (figures) and sources of information to which readers who need greater detail may refer. The illustrative models (the figures) are grouped in the second part. The third part consists of a combination of sources of information reflected in the first two parts, plus other sources of information, plus more detailed information relevant to the various sections in the first part. It is hoped that users of this guide will find in it sufficient information on each topic to determine whether or not they need more, and where to find more if they need it.

- 7 -
INTRODUCTION
The traditional birth attendant (TBA) has been defined as "a person (usually a woman) who assists the mother at childbirth and who initially acquired her skills delivering babies by herself or by working with other traditional birth attendants" (see note 1). In the light of evidence from various countries, it would appear that this definition of the TBA is rather narrow in the sense that, in many cases, the TBA's work includes not only her attendance at childbirth but the provision of basic care to women throughout the normal maternity cycle, the provision of care to the normal newborn, participation in the promotion of modern methods of family planning, and participation in other primary health-care activities, including the identification and referral of high-risk patients. Such referral is being increasingly assumed by TBAs in many countries.
The TBA, who is also known by other names, e.g., indigenous midwife, empirical midwife, traditional midwife, hilot, dunkun, and dai, is a familiar figure in almost every village and in many urban areas of Africa, Asia, and Latin America. It is estimated that, in the developing world, between 60% and 80% of all births are attended by TBAs.
In many countries there has been a laissez faire attitude towards TBAs, i.e., no attempt has been made to encourage, discourage, modify, or improve their practice. In a few countries the TBA's practice has been legally authorized under certain conditions. In yet others it is, at best, being tolerated until such time as the country can afford to maintain a sufficient number of professionally trained health workers to serve currently deprived populations. This may be an appropriate place to note that, in a number of developing countries, e.g., India and the Philippines, the problem is not so much the inability to train sufficient numbers of professional health workers, such as physicians and nurses, but the inability of the government to employ them productively in the health services. In the private sector, the purchasing power of large segments of the population is so low that they cannot afford, either directly or thro~gh social insurance schemes, the services of professional personnel whose education and, hence, utilization are costly. Moreover, most such health workers, once exposed through their training to the sophisticated technology and facilities of the teaching hospital, have little desire to work in less glamorous setting~ or to deal with the ordinary health problems afflicting the masses. The result is an excessive concentration of professional health workers in large cities and the emigration of those whom the cities cannot absorb. In either case, the vast majority of the people, particularly in rural areas, are deprived of even the basic elements of health care.
National administrations are becoming increasingly aware that, contrary to what was previously believed, economic growth - however rapid - will not on its own generate the momentum needed to improve the quality of life of the poor, and that health development is both a means to and a product of social and economic development, i.e., health cannot be achieved without development, and development is largely dependent on a healthy and productive population. In the light of this perception and of the imbalance that exists between health needs on the one hand and the resources available to meet those needs on the other, national administrations are exploring alternative approaches to meeting the basic health needs of people - approaches that depend neither on the building of costly hospitals nor on the provision of sophisticated services by personnel trained at exorbitant cost. In this regard, greater attention is being focused on ways and means of involving people in their own health care and of recruiting people from communities and training them to provide health care in the communities where they live and work. Additionally, evidence of the successful blending of traditional and modern medicine, such as has occurred in China, for example, and the findings of numerous anthropological and other studies of traditional healers have raised questions in the minds of many as to whether scientific health services are the only way to health.

- 8
All these developments have contributed to a re-examination of the role and practices of TBAs and to a consideration of how their current practices could be improved, what additional tasks they might be able to perform, and how the services of TBAs could be "articulated" (see below) with those of the organized or formal health services.
Allusion has been made at times to the notion of "integrating" the TBA into the organized health system. This has been viewed with mixed feelings of enthusiasm and trepidation. Integration has been openly enunciated and discussed in several countries, but as yet there is no known systematic framework for this. If by integration is meant that TBAs should be so intimately connected to the organized health system that they finally lose their identity as perceived in the traditional sense, this might well lead to conflict between TBAs and other categories of health personnel in the organized services, as well as between TBAs and the communities they would be expected to continue to serve. Integration in this, the true, sense of the term should be avoided at all costs, since it would defeat the purpose of programmes to extend health services to underserved populations. In order to ensure that the identity of the TBA remains intact and that the TBA continues to serve the community, only informal and flexible links should be developed between her and the organized health system. Thus, the question should not be one of defining the role of the TBA in the modern system of health-care delivery but one of defining the role that the modern system can play in helping TBAs to perform more safely those tasks they generally perform on the basis of the principles of mutual help and humanitarianism. In this context, the concern should not centre on integrating the TBA into the modern system but rather on ensuring that, within the TBA as a person, modern and traditional concepts and modes of practice are so integrated as to eliminate only traditional practices and rituals that are clearly shown to be harmful, and to instil only modern concepts and techniques that are absolutely essential to the safety of the persons under the care of the TBA.
For the above-mentioned reason, those who have been closely involved in the preparation of this guide decided to use the term "articulation" rather than "integration". "Articulation", according to Webster's Dictionary of Synonyms, "implies organization in which each part fits into another in a manner comparable to the fitting into each other of two bones at a movable joint and a structure so built that it functions as a whole yet without loss of flexibility or distinctness in any of its component units or without any conflict between them".
The guidelines presented in this document are intentionally limited in the sense that they are not meant to provide guidance either on how the government of a country should go about arriving at a decision to improve the skills of and to utilize TBAs as a component in the drive for greater coverage of the population with basic health care, or on how health planners should go about preparing a national health plan, a health manpower plan, or a plan for maternal and child health. The guidelines thus assume certain preconditions, among them the following:
(a) that the government has made a definite decision to take the necessary steps to involve TBAs more effectively in programmes to ex+~nd health services to underserved populations, and that this decision reflects eith~. the fact that there exist no strong pockets of resistance to the implementation of such a decision or the fact that the government is prepared to do what is necessary to overcome such resistance if it exists;
(b) that a health manpower survey has been carried out;
(c) that a survey has been made of organized health programmes and services currently provided - where they are, the agencies involved, the purposes they serve, what the staffing patterns are, etc.;

- 9 -
(d) that the health situation has been analysed, particularly in rural areas, and that priorities for health care have been determined.
The conditions listed above should exist prior to any move to embark on a nation-wide programme. This does not mean, however, that programmes cannot be developed in parts of a country where the necessary information exists as regards nealth manpower, health services, and the health situation, and where the means of communication and transport are sufficient to meet the needs involved in the training and supervision of TBAs and the referral of patients. Where these conditions do not yet exist, efforts hould first be made to bring them about. However, guidelines in those respects fall outside the scope of the present
publication.
The guidelines presented herein deal with a process that begins after a decision has been made (at whatever level) to extend services in maternal and child health and family planning to underserved populations by training TBAs and articulating their services with those of the organized health care system. At the same time, while a decision to train and use TBAs should be based on a realistic appraisal of the health/health-manpower/healthservice situation, it should not have to await either an inventory of TBAs or more precise information about the cultural patterns of individual communities and about the practiaes of TBAs. These are matters that can and should form a part of information-gathering and decision-making at later stages and perhaps lower administrative levels of programme develop-. ment and management.
1. OVERVIEW OF PROGRAMME PIANNING AND DEVELOPMENT
The first step in the implementation of the decision to develop a TBA programme should be the appointment of a senior person to be responsible for the planning and management of the programme, that person to be assisted by a small group of qualified personnel representing various disciplines. The first task of the group would be to formulate basic policies regarding the programme. The second would be to formulate and implement (with the collaboration of senior regional, provincial, state, and district personnel) a promotional campaign to inform and enlist the cooperation of members of the health professions, the TBAs, and the communities served by TBAs. The third task would be to formulate and implement (again in collaboration with other levels of health administration) a plan for gathering and analysing data on currently practising TBAs, current beliefs and practices of the community and of TBAs concerning maternal and child health and family planning, and existing programmes and services in maternal and child health and family planning.
On the basis of the data compiled and in the context of the basic policies defined at national level, the next step would be the planning and development of the training programme, broad guidelines for which would be formulated at national level and more detailed plans worked out at the regional, provincial, and district levels. The first task in this respect would be to define precisely the functions and tasks that TBAs would be expected to undertake, This would be followed by the selection and preparation of trainers, the selection of trainees, the development of learning objectives and of course content and methods, decisions as to how, when, and where the courses will be given, implementation of the training course and evaluation of the learning achieved by TBAs.
In parallel with the planning and implementation of the training programme, plans should also be made for linking the TBA's services to the organized health services, consideration being given to the orientation of health agency staff to their roles and responsibilities vis-a-vis the TR~, the supervision and continuing education of the TBA,

Phase I
Phase II
PROCESS FOR THE DEVELOPMENT AND EVALUATION OF PROGRAMMES FOR THE TRAINING AND ARTICULATION OF TBAS
Phases or steps
Preconditions
Policy formulation and promotion
Formulation of basic policies
Promotion of basic policies
Information gathering and analysis
On MCH and FP services and programmes
Inventory of TBAs
On beliefs and practices of the community and TBAs concerning MCH and FP
Explanatory remarks
(a) Decision to train and use TBAs (b) Health manpower survey (c) Survey of organized health programmes/services (d) Analysis of health situation
Concerning: (a) Functions., tasks, and technical procedures that TBAs
would be authorized to undertake (b) Drugs, supplies, and equipment that TBAs would be
authorized to .use or dispense (c) Broad teaching or learning objectives (d) Teaching or learning methods and materials
Through campaigns addressed to: (a) Health professionals (b) TBAs (c) The community
Network of MCH and FP programmes could serve as a mechanism for data collection in the next two activities and for subsequent training, supervision,and evaluation of TBAs
Could be carried out simultaneously with the next activity and through a single mechanism (see remark above)
(a) Preliminary enquiries needed for preparation of survey questionnaires
(b) Survey questionnaire for TBAs (c) Survey questionnaire for mothers
Illustrative models
Fig. 1
Fig. 2
Fig. 3 & 4 Fig. 5
...... 0

Phase III
Phase J.V
Phase V
Planning, development, and evaluation of the training programme
Preparatory activities
D0velopment of the course
Implementation of training programme
Evaluation of teaching and learning
Articulation of TBAs' activities with the organized health system
Programme evaluation
Assessment of numbers of TBAs trained
Assessment of performance of trained TBAs
Assessment of trained TBAs' impact on health status
(a) Specification of TBA functions and tasks (b) Selection and preparation of tutors (c) Selection of TBA trainees
(a) Pretesting of TBAs' knowledge, skills, and attitudes in relation to specified functions and tasks
(b) Specification of learning objectives on the basis of TBAs' deficiencies in knowledge, skills, and attitudes relevant to specified functions and tasks
(c) Development of course content and methods on the basis of learning objectives
Decisions (on the basis of discussions with TBA trainees) concerning time, place, and other aspects of the training programme
(a) Evaluation of trainees' learning (b) Evaluation of teaching and learning materials and (c) Evaluation oJ teachers (d) Evaluation of learning objectives
(a) Orientation of staff of organized health system (b) Supervision and continuing education (c) Supporting services (d) Records and reports
(e) Regulation of TBAs' practice
In terms of: (a) Quality of serv.ices provided (b) Quantity 6f services provided
In terms of impact on:
(a) Maternal mortality ) (b) Infant mortality (c) Disease among mothers (d) Disease among children
methods
Fig, 6
J~lg. 7, 8, 9, & 10 Ji'i.g, 11 & 12
Fig. 13, 14, & 15
Fig. 16
Fig. 17 & 18
Fig. 18

- 12 -
supporting services, records and reports, and the regulation of the TBA's practice. Pr~grallUlle evaluation in terms of the qu~ntity and quality of services provided by trained TBAs and the impact of such services on. the heal th status of mothers and children is the final phase of the programme.
The above is a simplified outline of the process involved, which is ~lso depicted in the model in the foregoing tabulation. It should be noted, however, that the process is not as linear as either the outline or the model suggests, since some components of, for example, the training programme can be planned only after other components have been implemented. The same applies to the process o'f linkage as it concerns the various components of that process and as it relates to the training programme.
2. FORMULATION OF BASIC POLICIES (GROUND RULES)
Once a decision has been made to train and use TBAs as a me~ns of extending health and family planning services, responsibility for the planning and implementation of the programme should be delegated to a senior person in the ministry of health, preferably one who was involved in the assessment of the health situation in the country and in the decision to train and use TBAs. A small group of people should be appointed to assist this person. The group, a form of national committee,- should reflect not only a variety of disciplines but also the best-qualified id each discipline. In this regard, consideration might be given to the inclusion of: a person who is highly knowledgeable about t.he country's health services; a medical officer; a nur~e/midwife educator, a social scientist; a member of the planning unit of the ministry of health; a pe-rson knowledgeable -about the work of TBAs (if possible, a TBA. as such); a representative of the consumers of health services; a mass medi.a expert; a management consultant; and a demographer.· To - the extent possible, the group should include selected_ personnel from organizational structures concerned primarily with the provision of maternal and child. health and family planning services.
The composition of the group at central level is likely to vary in accordance with the needs for expertise during the different stages of progr~mme planning, implementation, and evaluation. During the initial stage of planning, the group should consist of the persons who are bei;t qualified to carry out the first .task to be undertaken, namely, to define policy regarding:
the fune:tions and tasks thaCthe trained TBA wil.l :be authorized to.undertake;
the technical. procedures th.at the TBA will l)e author.ized to perform;
the broad areas of content to be included in the training programme for TBAs and guidelines for the development of content, including broad teaching and learning objectives;
the types of drugs that the TBA will be authorized to dispense; and
the supplies and equipment- that the government will make available to TBAs.
The policies defined by the group should be vie~ed as the ground rules upon which the programme would be elaborated and as the startirig point for-discussions, data gathering, and other activities at central, intermediate, and peripheral levels of health administration.

- 13 -
The functions. and tasks to be outlined at the central level should be limited to those that the trained TBA would be officially authorized to undertake, and should thus constitute a "maximum" list on the basis of which senior staff at intermediate and peripheral levels of health administration could;
(a) make decisions as to which of the functions and tasks authorized are pertinent to the needs of the administrative area concerned; and
(b) elaborate in greater detail the functions and tasks that are pertinent and feasible in the light of conditions obtaining in the administrative area concerned, e.g., the health problems and priorities~ the other categories of health workers available, the accessibility of health facilities, and the educational level of the TBAs.
The primary functions of trained TBAs should probably include· the provision of basic care to women throughout the normal maternity cycle, the provision of care to the normal newborn, and participation in the promotion of modern family planning methods. If the TBA is authorized to undertake other primary health care activities, these should be clearly indicated, as should any data-gathering activities in which she might be able to participate. In establishing the maximum list of functions and tasks that the TBA will be authorized to undertake, the group at central level might consider the comprehensive list outlined in Fig.I.
3. PROMOTION OF BASIC POLICIES
The decision to train TBAs and to link their services to the organized health care system constitutes a major policy change in most countries. As with all change, this decision is likely to create a state of disequilibrium within the system. The roles of other health workers may need to be redefined and, accordingly, programmes for the training of such workers may need to be reoriented to new roles. Mechanisms will need to be developed for linking the new workers to the system. Perhaps most important, in some if not all countries, are the changes in attitude that may have to be effected if the program.me is to be realistically designed and successfully implemented. Among the most important needs in this respect are:
(a) acceptance by health professionals of the TBA as a legitimate health worker;
( b) acceptance by TBAs of the need for their cooperation with the organized health services;
(c) acceptance by TBAs of the need for additional training; and
(d) acceptance by the comlnunity of the new practices of the TBA.
The second step, therefore, would be to design and implement a promotional campaign to inform and solicit the cooperation of those likely to be affected by or otherwise involved in the programme. The broad design for such a campaign could be worked out by the committee at central level (with the assistance of a person versed in mass-media techniques), and the details elaborated, as suitable and feasible, at intermediate and local levels. In any case, the campaign cou~d start with;
(a) the transmission of information - via radio, television, newspapers, journals, or other forms of mass media - regarding the basic policies governing the prospective programme, together with a clear rationale as to why the government is embarking on such a programme; and

- 14 -
(b) written notices to provincial and district health officers and to provincial and district government officials informing them of the basic policies, requesting their cooperation in the further promotion and development of the programme, and suggesting steps that could be taken at provincial and district levels to promote and develop the programme.
The content and intensity of the promotional campaign will vary from country to country, depending on the extent to which those likely to be affected by the programme were represented in the government's decision to train and use TBAs for the extension of health services. The campaign should be directed, at the least, towards three distinct target populations that will be affected by the programme and whose cooperation is essential -namely, professional health workers, the TBAs themselves, and the residents of communities in which TBA.s practise.
3.1 Promotional campaign addressed to health professionals
The campaign to solicit the cooperation of professional health personnel may well need to take into account the probability that, for various reasons (see note 2), many such persons find it difficult to accept the TBA as a legitimate member of the health team. Where this is so, the campaign should take the form of a strong "consciousness-raising" effort in which the plight of underserved populations, particularly those in rural areas, and the responsibility that the organized health services must assume in the nation's effort to improve health in such populations are clearly spelled out. In this regard, the audience concerned should be apprised, in one way or another, of certain facts and figures Qsee note 3).
In planning the campaign it is essential to involve: leaders of professional associations (medical, nursing, and midwifery); senior officials in professional councils or other bodies responsible for the registration and practice of the various health professionals; senior educators in medicine, nursing, and midwifery; senior staff in the health services; and senior officials in all government departments or divisions concerned with the development of health services and health manpower. Methods that might be used include informal meetings, seminars, workshops, and staff meetings (depending on the composition of the group and the purpose for which its members are brought together), as well as information circulars; articles in newspapers~ professional journals, and other periodicals; and information programmes via radio and television.
3.2 Promotional campaign addressed to TBAs
The success of any programme to extend health services through the use of TBAs will inevitably depend on the willingness of TBAs to cooperate with the organized health services, to participate in the training programmes to be offered, and subsequently to effect changes in their mode of practice. Not infrequently, TBAs hold strong anti-establishment views and are suspicious of government overtures. This is understandable, given that in many countries the practice of midwifery by TBAs has been considered illegal and many TBA.shave probably encountered the hostility of professional health workers with whom they have come in contact. Where such is the case, a campaign to enlist their cooperation will have to be carefully planned and executed. TBA.swill have to be convinced of the government's good intentions; of the value, to them and to the community, of their learning newer concepts and techniques to help mothers and children in particular and the community in general; and of the benefit to them of consulting with other experienced practitioners.
In addition to the widespread publicity for the government's policies via newspapers, radio, etc., the strategy for enlisting the cooperation of TBA.s might include:

- 15 -
(a) discussions at the local level between community leaders and health centre staff;
(b) involvement of a representative of TBAs in the planning process at central and intermediate levels; and
(c) involvement of TBAs in the planning of the programme at the local level.
3.3 Promotional campaign addressed to the community
It is essential that all the influential persons or groups in the community (village) be given as much information as possible about the programme so that they, in turn, can inform others in the community and seek their cooperation. They should also participate in the planning and implementation of the programme. Political leaders in the community should be the first to be approached. Their agreement is essential to the planning of meetings and discussions with other members of the community, including TBAs. Continuing dialogue with community leaders is essential throughout the programme - from its inception through its implementation and follow-up (see note 4).
4. INFORMATION-GATHERING FOR PROGRAMME DEVELOPMENT
Within the framework of the ground rules established at central level, definitive policies and plans will have to be elaborated regarding such matters as the precise tasks that TBAs will be expected to perform, the type of training they will need in order to carry out the tasks specified, criteria for the selection of candidates for training, criteria for the selection of trainers, the manner in which the practice of TBAs will be regulated, and the manner in which the services of TBAs will be linked to the organized health care system.
In order to develop policies and plans that are sound, rational, and capable of being implemented, those responsible will need certain basic information. It would be impracticable, for example, to have a policy that stipulates the ability to read and write as one of the requirements for entry to the training programme, if the majority of TBAs in the country are illiterate. Nor can the objectives and content of training programmes be realistic if no account is taken of the present practices of TBAs and how these fit into the cultural patterns of the communities in which they work. Additionally, a thorough knowledge of the existing services in maternal and child health care and family planning is essential to those determining how and where TBAs will be linked to such services. Basically, then, decision-makers will need information about:
(a) the structure of existing and planned health services in maternal and child care and family planning;
(b) the present pool of TBAs in the country - who and where they are and their basic characteristics; and
(c) cultural patterns, particularly beliefs and practices concerning the maternity cycle, infant and child care, and the spacing of children, and the beliefs and practices of TBAs in these respects.
4.1 Information on maternal and child health and family planning services
Information about the existing structure of services in the field of maternal and child care and family planning would serve at least three important purposes:

- 16 -
(a) it would help planners to decide how and where the services of TBAs could best be articulated with the organized health care system;
(b) the structure itself could serve as the mechanism through which other information needed for planning the programme for TBAs could be gathered and processed; and
(c) staff within the structure are the most likely of all personnel in the health systera to be aware of needs in the area of maternal and child care and family planning, and thus would be the most appropriate for developing the programme for the training and use of TBAs and their articulation with the organized health system.
In view of these considerations, the compilation of information on maternal and child health and family planning services should precede other data-gathering activities. Much of the relevant information is already available in some countries and simply needs to be brought together and organized for the purposes listed, above. Responsibility for this work could be part of the functions of the person at central level who is delegated to supervise the TBA programme. The planning unit in the ministry of health might be the most suitable for carrying out the work to be done in this regard, which would involve, as a first step, a search for answers to questions such as those listed in note 5.
4.2 Inventory of TBAs
For the effective planning, implementation, and monitoring of a TBA programme it is essential to have certain baseline information on curr.ently .. practising TBAs. In countries where such information is not yet available a survey will be needed. For countries interested in undertaking a nation-wide survey, the one carried out in the Philippines can serve as an excellent example. The report of that survey details the procedures involved and includes all the forms used. It is essential reading for anyone planning a similar survey at national level, and would also be a very helpful guide for the planning of surveys at sub-national levels. (See note 6 for further observations concerning the survey in the Philippines.)
The basic questionnaire used in the Philippine survey is reproduced in Fig. 2. At this stage of operations it is not necessary to collect all the information shown in Fig. 2. Much~of it could be collected as part of the information sought in the survey of local beliefs and practices, which is the subject of the following sub-section. Alternatively, the two surveys could be combined and carried out through a single mechanism, i.e., the network of services and programmes for maternal and child health and family planning, which was the subject of section 4.1.
It is usually not difficult to trace TBAs. The sources of information that have been used include c.ommuni ty leaders and officials, local heal th ce.ntres, and women who have recently given birth. Once some of the TBAs have been located, they can be asked to give details of others.
In the process of tracing and recording information on TBAs, it is important to anticipate the possibility that they will assume they are going to be harassed or even punished (see note 7). Problems of this kind are less likely to occur if interviewers are carefully selected, preference being given .to health staff who have had considerable contact with TBAs or whose work implies a link with that of TBAs. Others who could provide valuable assistance in the conduct of the survey are young people in rural communities who have completed nine or more years of general education.

- 17 -
All who are expected to be involved in the conduct of the survey should be properly briefed - well in advance of the implementation date - as to the reasons for the survey,
.the manner in which it will be conducted, and their role and responsibilities with respect to it. Local communities must also be prepared. In some areas it might be appropriate to ask a local leader to invite TBAs to attend an informal meeting with health service personnel to discuss the survey, including the role that the TBAs can play in ensuring that the objectives of the survey are achieved. It would probably help if the meeting were made something of a festive occasion, as is generally the custom with rural events. This meeting should reflect a real dialogue between TBAs and health service staff, rather than a situation in which the latter merely talk to TBAs.
The survey of TBAs, whether conducted separately from or together with the survey of beliefs and practices, should include information necessary for the development of a permanent register which, if kept up to date, can serve as an important source of information for continuous programme evaluation and planning. (See section 7,6 concerning registration.)
The survey of TBAs, like the survey of any target population, can be no more effective than the plan on which it is based. Those given the responsibility for planning and directing the survey should be capable of assuming responsibility for activities such as those listed in note 8.
4.3 Information on local beliefs and practices
Each society has its own customs, beliefs, values, and practices regarding birth and death, pregnancy, the care of mothers and children, and the spacing of children. These vary not only from country to country but among subcultures within a heterogeneous society. The practices of TBAs are rooted in the particular community in which they work, but variations in specific practices are also to be found among TBAs of the same community.
In a number of countries, a considerable amount of information has been gathered about social and cultural characteristics of communities. In each such country, a first step at this stage of operations might be the appointment of someone (preferably a sociologist and/or anthropologist) to be responsible for drawing together the existing literature (published and unpublished) on the subject as it pertains to the country and particularly to maternal and child care and family planning. Some, if not most, of the information may have been collected by individuals and agencies outside the country, and thus appear in books and journals published outside the country. Thus it would be necessary for a thorough bibliographic search to be made, the relevant literature collected and examined, and such information extracted as would be useful for planning, implementing, and evaluating the programme for the training and use of TBAs.
In countries concerni'ng which there is little relevant documentation, a sociological study would be in order. The cooperation of the sociology department of the local university would be of great value in this regard. In countries where a survey of TBAs such as that described earlier is envisaged, it might save time and money if the pertinent sociological data were collected through the mechanism established for the survey. Thus, in addition to the basic data needed for the survey of TBAs, interviewers might also seek data that would help planners to:
(a) identify aspects of traditional practice that nead to be changed (and thus need r,o be taken into account in the training program.~e) in order to secure a significant improvement in maternal and child health;
(b) gauge the extent to which TBAs would be amenable to receiving training, cooperating with the organized health servir:.es, a:-:.d participating in family planning progr2.mmes; and

- 18 -
(c) gauge the incentives that may be needed to obtain their cooperation.
The types of information that interviewers might seek in order to help planners in the above-mentioned tasks might include the following:
(a) the particular techniques, rituals, and procedures that the TBA performs and the nature of the advice that she provides in connexion with her work with mothers and children (in this regard it would be important to ascertain the extent to which certain practices of the TBA reflect her personal beliefs and values as opposed to those of the community);
(b) the views of TBAs and others in the community as regards modern contraceptives, child spacing, and family size;
( c) how the TBA feels about receiving training and cooper a ting w'i th the organized health services;
(d) how the people in the community acknowledge the status of the TBA;
(e) how the TBA is remunerated for her work, how she regards that remuneration, and whether she would expect payment from the government for her cooperation with the organized health services;
( f) whether the TBA would be interested in becoming a trai.ner of TBAs;
(g) how the TBA views the notion of her assuming other tasks in primary health care; and
(h) what major problems the TBA faces in her health-related work in the community.
4.3.1 Preliminary enquiries
The value of the findings of a formal questionnaire survey are heavily dependent on the information that goes into the preparation of the survey. In this respect, the survey is like the everyday experience of trying to obtain information from a stranger. For example, if a stranger is from a developed country, it is generally a simple matter to find out from him the year of his birth. Much more prior information may be required in the case of an individual in a society where it is not customary to keep written records of such events as births. In his case, it might be necessary first to discover the dates of impor-tant events in the history of his community, so that it would be possible to ask him when his birth occurred in relation to these. (In fact this is a common tactic for census enumerators in some developing countries.) When the types of information required are of the kind listed above, the problem is much more complex and an abundance of prior information is needed if the survey is to accomplish its purposes. The information should encompass all the topics that the survey will investigate. Ideally, the following information is required in ad~ance of the survey:
a description of the local role and status of the TBA;
an inventory of local beliefs and practices; and
enough knowledge of the local linguistic usage to permit the framing of questions that will elicit valid data on all the topics of the survey.

- 19 -
If health service personnel are familiar with the area, much of the required preliminary information is likely to be available from them. It is also worth investigating the possibility of involving anthropologists in the enquiry. They can be very helpful as investigators and interpreters of local knowledge and practices. In a project in Central Java, an anthropological enquiry provided much of the preliminary information needed for a survey of TBAs' attitudes to the prospect of acting as agents of the national family planning programme (see note 9). In an anthropological enquiry in the Philippines, one of the topics studied was the indigenous theories used by Filipino peasants to rationalize their behaviour and experience, including their reproductive behaviour and experience. Clearly, where actions are guided by theories such as those described in the report of that enquiry (see note 10), it is important that their prevalence should be investigated by the formal survey. If the survey is to do this effectively, it needs to be based on adequate preliminary information about the nature of indigenous theories.
4.3.2 The survey questionnaire for TBAs
A questionnaire survey can extend the information obtained through the inventory of TBAs. In a small area, efforts should be made to seek the necessary information from all TBAs in the area. In the case of a large area, a representative sample may be more feasible. In either case, the objective would be to find out what the TBA already knows and can do (or conversely what she does not yet know and needs to learn) as a basis for defining training objectives and developing course content. The data from the questionnaire may also serve as baseline data against which subsequent changes in the knowledge, skills, attitudes, and behaviour of the trained TBA could be measured. Fig. 3 shows a questionnaire prepared for use in the Philippines. Fig. 4 shows one prepared for use in Mexico (see also note 12). These questionnaires differ primarily in two respects: that for the Philippines is highly structured in format and is focused exclusively on the knowledge and practices of TBAs, while the one for Mexico is open-ended and seeks both social and demographic data on the TBA and data on her knowledge and practice.
4.3.3 The survey questionnaire for mothers
Responses to the survey questionnaire for the TBA will not provide all the information required. In particular, they will not reveal what her clients think of her practices, or why they often do not use modern services even when these are available. To obtain such information, it is necessary to interview a sample of women in the country. In Mexico, in addition to the questionnaire for TBAs mentioned above and shown in Fig. 4, a questionnaire was also prepared for use in obtaining information from mothers. This is shown in Fig. 5 (see also note 13).
The manner in which questionnaires are administered influences considerably the results obtained. Great importance is attached, therefore, to the need for meticulousness in the selection and training of interviewers, in the designing of the interview schedule, and in the preparation of the population within the survey area to cooperate in the study. An example of a survey in which particular attention was paid to these factors is the survey of women in a tribal community in central India (see note 14).
4.3.4 Shortcomings of questionnaire surveys
Some questionnaire surveys of TBAs have created expectations which later proved to be unrealistic. For example, according to an account of a survey of TBAs in a local area of one African country, 80% of respondents indicated that they approved of couples doing something to postpone pregnancy so they can have the number of children they want, and 73% felt that women in their village would be interested in family planning. of the performance of 30 trained TBAs in the area over a nine-month had recruited a total of only 19 family planning acceptors.
A subsequent evaluation period showed that they

- 20 -
The fact that questionnaire surv'eys in general (not merely surveys of TBAs) often fail to obtain valid and reliable data has received increasing attention in recent years. A summary of evidence on the failures of surveys of reproductive behaviour is presented by one writer ( see note 15), and a more genera.I review of the problems and some further evidence are presented by another (see note 16). While inconsistencies between su!vey evidence and actual behaviour are more prevalent in the case of surveys that attempt to obtain data on people's ideas, attitudes, and intentions, experience has also shown that surveys on people's behaviour and circumstances can also, at times, be very undependable sources of data.
There are several reasons for these shortcomings. Many respondents are reluctant to admit that they do not .know the answer to a question when the very fact that it is asked seems to indicate that "normal" people would have an answer. Another problem is the tendency of respondents to want to give stereotyped answers or ones they believe will be approved (see note 17). Often the type of answer sought by questionnaires (for example, "yes" or "no") does not give respondents an opportunity to reveal the often complex considerations (such as "but only if my husband agrees") which would be part of a full answer, The main problems of questionnaire design are usefully treated in a widely used introductory text by one writer (see note 18),
Many of the difficulties arise from the fact that interviewers are normally required to present questions to all respondents in the form in which the questions appear in the questionnaire. While this convention is very important for some kinds of survey, it seems to cause unnecessary difficulties for surveys of TBAs. As an alternative, where interviewers have the necessary techliical knowledge, they might_ be asked to discover, by informal questioning, which answer among predetermined alternatives best represents the respondent's answer to each item in the questionnaire, For example, interviewers might be asked to determine which of various alternative answers (the alternatives having been established by preliminary enquiries) best represents the respondent's answer to the question: "How do you kn'c>w when a woman is in labour?" Experience strongly suggests that the scope of questions should be restricted to topics concerning the TBA's knowledge, behaviour, and such characteristics as literacy level, and should not also encompass attitudes and intentions, A useful way of obtaining information on attitudes is to _hold group discussions of the kind described in section 6,2.
4.3.5 Sampling
Except for programmes confined to a very small area, it is impracticable to try to interview all TBAs or all their clients. The usual practicre is to interview a sample of individuals believed to be representative of the target population. Choosing respondents in a way that ensures a truly representative sample is often a complex task requiring expert assistance. However, the purpose of most TBA surveys can be adequately served by simple procedures. In many cases, it will be enough first to identify women who have given birth in the past year in a few typical rural communities, and then to try to interview either all the mothers identified or all the TBAs involved, or both. The total number of interviews that this procedure would require in a given set of communi_ties may be roughly determined from a knowledge of their population size and the birth rate in the area, It might also be useful to compare results from typical communities with those from areas that are atypical in some relevant respect, such as in their access to health services,

- 21 -
5, PLANNING AND DEVELOPMENT OF THE TRAINING PROGRAMME
Within the framework of the ground rules established at central level, and on the basis of the information derived from analysis of the data gathered, detailed plans for the training programme may be formulated, In some countries, the desire might be to develop a single national plan applicable to all regions or provinces. This may be feasible in countries that are relatively small in terms of geography and population, where the population is reasonably homogeneous in terms of language and other cultural attributes, where there is a rather uniform pattern of health problems, and where resources in rural areas - however limited such resources may be - are rather. evenly distributed in terms of numbers and categories of health workers and accessibility of health centres, In countries where the obverse obtains in the above respects, it would be preferable for the more detailed plans to be wo:rked out at intermediate levels of health administration, so that they may be more directly oriented to the particular needs of the region or province concerned and may, where necessary, be more readily adapted to the particular needs of individual localities within the region.
All groups of persons that are expected to be affected by the programme should have an, opportunity, through a representative, to voice their opinions and provide suggestions before the plans for the programme are made final. Draft plans might be circulated, for example, to professional associations, senior staff in health services, senior educators in the health field, one or more persons who can speak on behalf of the consumers, and one or more who can speak on behalf of TBAs. Under all circumstances, staff at peripheral levels of health administration should be consulted, since they are likely to be the most familiar with the conqitions obtaining in the locality concerned. As a corollary, under no circumstances should the planning of the training programme be left entirely to those who are unfamiliar with the localities concerned.
Aspects of the training programme to be considered include the following:· the TBA's function& and tasks, on which the training will centre; the specification of learning objectives; the selection and preparation of trainers; the selection of trainees; course content and methods; and the place, duration, and other aspects of the training programme, These are discussed below,
5,1 Definition of functions and tasks of TBAs
Within the framework of the functions, tasks, and procedures that the group at central level define as being those that the TBA will be authorized to undertake (see section 2) and in the light of the knowledge gained from the data gathered (see section 4), decisions will have to be made as regards the specific tasks that the TBA will be expected to undertake. These may vary from one geographical area to another, depending on, for example, the types and numbers of other health workers in the area concerned and the content of their work, the accessibility of referral facilities, the educational level of the existing pool of TBAs in the particular area, and the priority health problems in the area, In some areas, there may be good reasons for taking the view that it is unrealistic to expect a training programme to equip the TBA to undertake all the tasks shown in Fig, 1. Circumstances in other areas may permit a more optimistic view.
Particular attention should be given to defining the functions and tasks of TBAs in such a way that they complement rather than overlap those of other health workers. There is also the possibility that the functions and tasks of other health workers in the area may need to be redefined in the light of those defined for the TBA. The focus should be on deciding which category of health worker would be most suitable - and available - for each type of health work.

- 22 -
From the standpoint of evaluation, the clear specification of tasks is necessary as a basis for determining both the learning objectives against which individual performance is to be measured and the kinds of effect it is reasonable to expect the training programme to have on health status.
5.2 Selection and preparation of trainers
Those who are actually going to do the work of training TBAs should be intimately involved in the planning of the training program.~e in terms of learning objectives, content, methods, and location and duration of training. Thus, once the functions and tasks of TBAs have been defined, and before any attempt is made to refine content and methods, the next step would be the selection and preparation of trainers.
Collectively, potential trainers of TBAs might be drawn from, the following:
(a) local TBAs who manifest a potential as trainers;
(b) experienced educators or tutors in the area of maternal and child health and family planning; and
(c) individuals who are likely to be the direct supervisors of TBAs in the local area.
The questions as to who the trainers will be and how many will be needed will be of critical importance and will depend on how the training programme is viewed in the long term. If, for example, the government is committed to the development of self-reliance 'at the village level, every effort should be made to identify persons at that level who show potential as candidates for training as trainers. The focus should be on identifying each TBA who can read, write, and speak the language of the community (a prerequisite for any trainer, whether or not from the community concerned), who has had considerable experience as a TBA, who is respected by the community, who would be interested in becoming a trainer of TBAs, and who might find the time to undergo the teacher-training programme and, subsequently, the time to teach others. The information obtained via the inventory and the sociological study (singly or combined) would indicate TBAs who meet some of the above criteria. In countries where even a very few such TBAs are initially available, attempts should be made to provide them with the necessary training. This may mean the setting up of a special programme for them - one whereby they can learn;
(a) safe methods of practice (essential to their continuing work as TBAs and to their future additional work as trainers);
(b) methods of teaching (they will need help, for example, in understanding how the illiterate or semiliterate learn, devising methods that would enhance the durability of learning, defining objectives and content for specific teaching sessions, organizing teaching and learning materials, and identifying basic principles to be emphasized); and
(c) the essentials concerning health services available to people in their respective communities (with the number of services being offered, often by different agencies or various divisions of the ministry of health, it would be important for prospective trainers to have a good overview of the services available and how the TBA's work is expected to be linked with such services).
For those who have never taught before, the training programme will most probably be of longer duration than that for experienced teachers, and the learning objectives may also be considerably different. Whereas the programme for TBAs drawn from the local area

- 23 -
will need to focus primarily on the elements listed above, that for experienced teachers will need to focus on the knowledge they must have in order to adapt content and teaching or learning strategies to the requirements of learners who are different from their previous students in terms of age, educational level, and cultural background, Thus, experienced teachers may need orientation in regard to:
(a) the characteristics of TBAs and the ways in which they function in their community;
(b) the beliefs, customs, and values of social groups other than those from which they (the teachers) come; and
(c) the economic, environmental, and health conditions of people living in rural areas - as mentioned earlier, many health professionals are unlikely to have much first-hand knowledge of such conditions.
In order to gain first-hand knowledge regarding the above-mentioned points, it would be essential that those being prepared as trainers of TBAs spend sufficient time in villages from which the potential trainees under their charge will come. The knowledge they will gain from discussions with village leaders, the TBAs themselves, and others, and from their observation of physical conditions in the village, will be extremely useful in their later participation in the development of course content and methods suited to the needs of those they will train.
Decisions will also need to be made as to when and where the orientation programmes for trainers will be given, who will sponsor the programmes, and who will provide the orientation, In the case of trainers who are already technically competent in teaching and in maternal and child care and family planning, all they may need is sufficient time and money to cover the cost of their visits to villages in order to gain first-hand knowledge of conditions there, In other words, it may not be necessary to organize the more formal type of teachertraining programme needed for the preparation of potential trainers from among local TBA practitioners.
The number of trainers to be selected will depend on the expected number of trainees, the duration of each training course, the distance between the work site of the TBAs and that of the trainers, and the volume of other work with which trainers will have to cope, If a decision is made to the effect that training shall be conducted primarily in the localities where the TBAs work, this might entail considerable travel time on the part of individual trainers - time that would thus not be available for their other tasks. Training provided outside the health centre would, therefore, most likely call for a larger number of trainers or, alternatively, for personnel to assume some of the other tasks that previously had fallen to the trainer. (The book cited in note 1 provides additional guidelines on the selection and preparation of trainers and supervisors.)
5.3 Selection of trainees
To the extent possible, potential trainees should participate in the planning (at local level) of the training programme in terms of learning objectives, content, duration, time, and place of training, Thus, the next step would be to select the trainees, at least the initial group to be trained from each locality. For this purpose, policies will have to be formulated as to who will be trained and how the candidates are to be selected. In this regard, the following questions arise:
(a) Is the basic objective of the programme to improve the practice of existing TBAs, or is it to prepare others to replace existing TBAs - or both? It would appear to be more practical to focus first on improving the practice of existing TBAs. Some reasons for doing so are outlined in note 19.

- 24 -
(b) Who is in the best position to nominate candidates for the training programme? Village leaders should in all cases be contacted in this regard. It would also be important to have community participation in the selection of candidates as a way of laying the groundwork for the community's acceptance of the new practices that TBAs will learn in the programme. The names suggest~d should be checked against the inventory of TBAs in the area.
(c) Will all who volunteer for the programme be accepted? Theoretically, it might be advisable to accept all of them but, if the number initially volunteering exceeds the number that trainers can adequately deal with at the start of the programme, a timetable should be devised whereby those meeting all the defined criteria will have first priority, others entering the programme at later stages. Priority might thus be given, for example, to those who are between 40 and 60 years of age, can read and write, and have attended at least a specified number of births during the previous year. Before any selection campaign is started, the inventory of TBAs in the area should be scrutinized for clues as to criteria that might be used to guide the initial and subsequent selection of candidates. The TBAs themselves should be invited to suggest criteria, but without their having access to the inventory, the confidentiality of which should be strictly maintained. Special consideration should be given to TBAs who come from communities that have the least access to health services. In all circumstances, criteria should be flexible enough to allow most TBAs who so desire to undergo training at one time or another. At the same time, there should be a constant search for young persons in the community who might be trained for health work such as that expected of TBAs. Such persons, while not having the experience of TBAs, might have achieved a higher level of general education that would make them more receptive to new knowledge.
(d) Should special incentives be used to encourage TBAs to enrol in the training course? There are opposing views on this. If there has been an effective promotional campaign within the community, the approval of village members may constitute all the reward that is needed, together with the satisfaction that the TBA herself feels upon completion of the course. On the other hand, it has been demonstrated that learning is facilitated when there is some form of special award at the end. If it is decided that an incentive is needed, it may be helpful to consult with village leaders as to the type that would be most appropriate and acceptable in the eyes of both the TBAs and the <COmmunity. Various forms of incentive have been used. The awarding of a certificate upon successful completion of the course is one that has frequently been used; another is the kit, often that provided by UNICEF, which contains basic equipment and supplies for the TBA's work. Some programmes have provided a stipend or a salary for TBAs during the period of the course. If such is to be provided, the question of how, when, and by whom it is to be provided will have to be considered.
5.4 Development of the course
In a nationwide programme the development of a course for TBAs may be viewed as essentially a three-step process whereby:
(a) general objectives and guidelines would be established by the committee at central level (see section 2);
(b) selected educators and service personnel at the intermediate (regional or provincial) level would: define the objectives of the training programme in the light of the needs of the particular region; develop course outlines;

- 25 -
identify feasible teaching and learning methods and available materials; estimate the duration-of the programme and the length of training for each group of TBAs; and identify health institutions where training could be given; and
(c) trainers at the local level, in collaboration with community leaders and with potential trainees and their prospective supervisors - within the framework of
-(a) and (b) above - would work out the fine details of the training course (what, where, how, and when) so that the course may be tailored to the particular needs of the trainees and of the population in the local area concerned.
5.4.l Specification of learning objectives
Fer the purpose of this field guide, a learning objective is taken to mean what a WHO study group defines as "a statement describing the expected results of learning experiences as they manifest themselves in the performance or behaviour of the learner" (see note 20). The rationale for any specific learning objective is that there are sound reasons for believing that its attainment will materially increase the TBA's competence to improve the health status of her clients.
The functions and tasks that the TBA will be expected to undertake after her training should cohs~itute the foundation on which learning objectives will be specified and course content developed. It should be borne in mind, however, that even before training commences each TBA will possess a certain amount of knowledge, skills, and attitudes concerning some or many of the tasks concerned. It is essential, therefore, that those responsible for developing the training programme refrain from loading it with matters about which the particular group of TBAs concerned is sufficiently knowledgeab_le, To this end, it is important that they should do the following, in the order indicated:
(a) examine the list of functions and tasks expected of the TBAs;
(b) identify, through preliminary tests or surveys of TBAs and/or discussions iith them, the particular functions and tasks (or detailed aspects thereof) concerning which the TBAs appear to lack the appropriate knowledge, skills, or attitudes;
(c) specify learhing objSctives in the light of the deficiencies identified; and
(d) plan learning experiences geared to the learning objectives specified,
For ~lues as to the particular learning needs of trainees ln a sp~cific locality, the information derived from the data-gathering efforts suggested in section 4, and particularly from questionnaires such as those exemplified in Fig. 3 and 4, should be carefully examined. Additionally, it would be worth while to invite prospective trainees to express their views on such matters as those listed in note 21.
A WHO publication mentioned earlier (see note 1) contains a comprehensive list of hypothetical learning objectives for TBAs, covering practically the whole range of possibilities for learning. This li~t can be useful in several ways. For one thing, it can be useful for the designing of preliminary tests or surveys of the knowledge, skills, and attitudes that TBAs have prior to their training. For example, with respect to the training for antepartal care, the first hypothetical objective listed reads as follows: "At the end of this section the TBA is able ~o: (a) identify the location and functions of the female reproductive organs, both internal and external; ... ''. Those responsible for specifying

- 26 -
learning objectives should first decide whether that objective is relevant to the tasks the TBA will be expected to perform. If it is considered relevant, the preliminary test or survey should seek to find out whether the TBAs concerned are already able to identify the reproductive organs mentioned, If not, that particular hypothetical objective should become an actual objective, The same procedure is applicable to all the objectives listed in the publication,
Some specialists in education feel that it is useful if each learning objective is aligned beside a statement of the pre-training knowledge, skill, or attitude of the learner concerning the respective objective. For example:
Present knowledge Learning objective
Does not assign any significance to changes in the uterus, abdomen, and breasts during the p~erperium.
Is able to identify and interpret normal and abnotmal changes in the uterus, abdomen, and breasts during the puerperium.
The obvious advantage of this method of specifying learning objectives is that it is much more informative about the real nature of the teaching or learning task involved than is the conventional method of simply listing objectives, Furthermore, it may encourage trainers and programme administrators to take explicit account of TBAs' existing knowledge and practices, Because many practices of untrained TBAs are likely to be founded in local theory, it may also be useful if the underlying theory is mentioned as part of the statement of present knowledge and practice, since awareness of the theory itself may help the trainer to design a way of encouraging the TBA to abandon the practice concerned if it is known to be unsafe. This would apply, for example, to a TBA's practice of outlining the edges of the newborn's eyelids with kohl (a powder, usually antimony, used by women in the East to darken their eyelids), the rationale being to keep evil spirits away,
In cases where harmful practices reflect the cultural and religious beliefs and demands of the community, rather than solely the idiosyncrasies of the particular TBA, the latter may find it difficult to abandon such practices, in which case trainers will need to provide appropriate health education to the community, particularly the women.
In planning course content, every effort should be made to ensure that current practices of the TBA that are safe and beneficial (either physically or psychologically) to the patient are reinforced, that those that are harmful are abandoned, and that those that are harmless are ignored. The effects of some practices have not been ascertained, These require further investigation, It is interesting to note, for example, that in some countries TBAs have traditionally used spiders' webs for dressing the umbilical cord. Initially, most Western physicians viewed this as a dirty and dangerous practice, but it was later shown that spiders' silk (and saliva) has antibiotic properties - a fact that TBAs had apparently recognized for years,
At a consultation on the role of the TBA, held at WHO headquarters in 1973, a group of public health nurses and other specialists from various countries drew up a list of existing practices and set against it a iist of proposed modifications and additions (see note 22). The result is shown in Fig. 6, Subsequently, some participants in the meeting vigorously opposed the list of modifications, arguing that the prescriptions were totally unrealistic, This argument notwithstanding, the list has the merit of illu_strating the ideas of treating learning objectives as modifications and of showing the range of existing practices,
A recent WHO publication provides, inter alia, detailed guidelines concerning the specification of learning objectives (see note 23). It states, for one thing, that each objective must be relevant, logical, unequivocal, feasible, observable, and measurable.

- 27 -
5.4.2 Other aspects of the training programme
In addition to the development of learning objectives and course content, a number of other aspects of the training programme will need to be considered, e.g., the number of trainees to be enrolled at each stage of the training programme; the duration of training for each group of- trainees; the duration of each training or learning session; the teaching and learning methods and materials to be used; and the place where the training will be given. The nature of the programme in these contexts will be dictated largely by practical considerations such as those listed in note 24.
6. EVALUATION OF THE TRAINING PROGRAMME
The discussion that follows focuses on ways of measuring the immediate effects of the training programme on the knowledge, skills, and attitudes of the TBA, as well as on the evaluation of learning objectives, teaching materials and methods, and the trainers themselves. (Section 8 will focus on evaluation of the trained TBA's performance in the community and of the impact that her work has had on the health status of the population served by her.)
The learning objectives specified constitute the common denominator for the evaluation of the various components of the training programme, i.e., students, trainers, materials, methods, and the learning objectives themselves.
6.1 Evaluation of the trainee
Techniques for evaluating the learning of students are not limited to the usual penciland-paper tests. In the case of TBAs, many of whom are illiterate, such tests will naturally be the least effective. The nature of the techniques used will influence the type of learning that goes on in the classroom. If students are constantly evaluated on subject matter alone, i.e., if they are asked merely to define, list, and describe certain factors, their learning efforts will focus on memorizing what is necessary to this end rather than on understanding. The method of teaching will also be such that it encourages students merely to memorize, In other words, the type of evaluation device used determines, to a great extent, the type of teaching and learning activities that go on in the classroom.
The methods of evaluation chosen should, of course, be appropriate to the learning objectives concerned. When the objective calls for the ability to recount facts, some form of oral or written test is indicated. On the other hand, tests of practical skills and, in many cases, tests of the understanding of principles, call for practical demonstration on the part of the student and its observation on the part of the te~cher or supervisor. Often, as in the example shown below, both types of test are appropriate. In general, the more tests used for each objective, the better.
A widely used textbook on the measurement of learning (see note 25) recommends the preparation of a "test blueprint", i.e., a document in which learning objectives are listed and, in relation to each, the appropriate course content and the methods by which the trainees' competence is to be measured. A WHO manual for the training of primary health care workers (see note 26) goes a step further by suggesting the arrangement, in columns, of information relating to: learning objecti\-es; finding out what the trainees already know about the problem; the major elements of content with regard to what the trainees must know and what they must do; using what the trainees have already learned; the teaching and learning methods to be used; and the methods of evaluating learning. The manual contains two examples of such a model. One of these, which concerns the problem of the badly fed child, is reproduced as Fig. 7.

- 28 -
The best way of determining whether a TBA has attained her learning objectives is to observe what she actually does. She can be observed in classroom simulations of practice (including responses to simulated emergencies) and when she attends deliveries under supervision in the local health centre and in the homes of her clients. Details of the observed performance may be recorded on a standard form, for evaluation purposes and as a basis for remedial teaching if required. Fig. 8 shows a sample checklist to assess the TBA's performance during a delivery demonstration in the home. Fig, 9 shows a sample checklist for the assessment of the trained TBA• s use and care of the delivery kit.,
In many situations, informal discussion is likely to be the only feasible way of discovering changes in the TBA's attitudes and knowledge. The principal advantages of this method are that it is a more natural way of communication and that it circumvents the problem of trying to devise standard questions that mean the same to all trainees. If,
however, the trainees are sufficiently literate, they could be set a written examination. More usually, training personnel read the questions of a formal .test to trainees, and record their answers. Fig. 10 shows an example of a formal test used in a .training p_rograrnrne in Mexico.
In teaching and learning activities and in testing, efforts should focus on encouraging TBAs t.o use all five senses (sight, hearing, touch, taste, and smell). The last two are particularly important in the case of TBAs who are illiterate and therefore cannot read the labels on various medicaments that they will be expected to use in their practice. Since labels on containers of medicaments often disappear and the writing thereon sometimes is or becomes illegible, the need for all TBAs to be able to recognize certain,medicaments by taste or smell becomes essential.
_Tests of. knowledge may be used at the start of training and at various stages duripg the course. Frequent ~hort tests, of whatever kind, are preferable to infrequent, long .tests. The former are less likely to cause anxiety to trainees and are useful in revealing the need for remedial teaching during a cour?e.
0 Any test that normally takes longer than half an
hour is too long for trainees to .whom any kind of test is usually an unfamiliar experience. On the _other hand, the trainee should be given as long as she wants to complete the test. For TBAs, .ability to complete the test in a specified period should not be regarded as part of the test.
In the preparation of questions for .a formal test, it is helpful if each .one is written on a separate card or piece of paper. Questions can then be more easily revised, removed, or re-arranged. If questions for these tests are to serve the.ir purpose, their formulation requires _considerable care. Leading questions and questions in a form. that enables the trainee to guess t.he desired answer (e.g., "Do you approve of family_,planning?") are obviously not satisfactory, nor are those that use unfamiliar terminology and those that elicit not evidence of understanding (when this is wh.at is sought) but merely evidence of ability to recall the correct response.
6.2 Evaluation of teaching and learning materials and methods
It is almost always possible to improve the trainee's performanc(;l by improving the quality of training. For this reason, _the evaluation of teaching and learning materials and methods sho_uld r_eceive regular attention, particularly in cases wl,ere a considerable proportion.of the trainees fails to attain the learning objectives.
The teaching materials produced for TBA training programmes sometimes include· a manual. Most manuals rely heavily on the printed w~rd, and some have no illustrations at all,. which presumably limits their value to the many TBAs who are either illiterate or whose ability

- 29 -
to read is limited, One exception is the manual of illustrations produced for TBAs in the Philippines, A page from this manual is reproduced as Fig, 11. Another manual that contains many useful illustrations is that prepared by WHO for the training and use of primary health care workers, including TBAs (see note 26). A page from that manual is reproduced as Fig. 12.
One way of evaluating teaching and iearning methods and materials is to analyse the results of tests taken by trainees, to discover mistakes and misunderstandings that better materials and methods might help to reduce. Alternatively, it may prove worth while to explore, through discussions with and among .the trainees, not only their understanding of what they are expected to learn f-rom specific parts of a manual, or from a demonstration or a lecture, but also the significance that they attach to the matter learned. It might happen that they manifest a perfect grasp of a technical point but, at the same time, considerable scepticism about its relevance. The discussion leader should be someone whose status and personality encourage frank discussion. might become an instructive teaching aid,
6.3 Evaluation of the trainers
If the discussion is recorded, the tape
The procedures reviewed above for evaluating teaching and learning materials and methods may also reveal ways in which some trainers are more competent than others, and perhaps ways in which trainers as a whole might improve. The TBAs themselves are the best source of information on trainers' patience, their respect for the trainees, their sensitivity to the problems of the trainees, and their commitment to the programme, Comparisons of the performance of students taught by different persons in the same programme may be used to encourage less effective staff to make greater efforts, Comparisons between different local programmes may also be useful in this respect,
6.4 Evaluation of learning objectives
As indicated at the end of section 5.4,1, a learning objective must be relevant, logical, unequivocal, feasible, observable, and measurable, In programmes where the TBAs' standard of performance in relation to any specified objective is below that expected, the objective itself should be re-examined with respect to each of the criteria mentioned above.
7. ARTICUIATION OF THE TBA'S ACTIVITIES WITH THE ORGANIZED HEALTH SYSTEM
In parallel with the development of the training programme, plans will have to be made regarding the manner in which the services of trained TBAs are to be articulated with those of the organized health services. The health agencies concerned will probably include rural ( or local) heal th centres· and/ or midwifery, puericul ture, and other clinics that operate at the rural (or local) level, as well as district health services, including both hospital and community (or public health) agencies, If there is a rural (or local) hospital, this also will be included (see also note 5). Consideration will have to be given to such matters as:
the orientation of staff as regards their role and responsibilities vis-a-vis TBAs;
the supervision of TBAs after their training;
the supporting services that will be required;
the records that will be needed;

- 30 -
the relationship of TBAs to other workers in the village, at the rural (or local) health centre, and at the nearest hospital; and
the regulation of the TBA's practice.
7.1 Orientation of staff
The attitudes of staff in the health agencies - both those who will be in direct contact with TBAs and those who will be responsible administratively or otherwise for dealing with people referred by TBAs - will be of crucial importance to the success of the programme. Attitudes tend to flow downwards in any organizational structure, i.e., people at lower levels tend to take their cues from people in more senior positions. It is essential, therefore, that a special effort should be made to gain the support and cooperation of senior staff in the health agencies concerned. To the extent possible, however, all staff at the district and local health centre, as well as those in charge of emergency units at the nearest hospital, should be involved in decision-making regarding not only the administrative arrangements (supporting services, supervision, records) for linking the TBA with the centre or hospital but also their role and responsibilities with respect to the TBA. To this end they will need to be informed about the role and functions of trained TBAs and about the training programmes.
The immediate supervisors of TBAs, particularly when they are persons other than the trainers of TBAs, will need a more comprehensive orientation than that provided to staff who are less directly concerned. They will need more detailed information about, for example, the tasks that TBAs under their supervision are expected to undertake and what exactly the TBAs have been taught. They will also have to be apprised of the precise nature of their own supervisory functions vis-a-vis the trained TBAs and, if they have not had training for particular supervisory functions, they should receive the necessary training. For example, if TBAs are expected to participate in family planning programmes, the supervisor will need to be prepared to provide the necessary supervision in this area of work. If possible, the supervisor should attend the course given to TBAs. In any case, liaison between staff who train TBAs and those who will supervise the trained TBAs is essential if coordination and follow through of the programme are to be ensured.
7.2 Supervision and continuing education of the TBA
The supervision of trained TBAs will constitute the major link between them and the organized health services. Therefore, a detailed plan for supervision should be established -one that indicates clearly the objectives of supervision, the persons who will provide it, the manner in which it will take place, its content, and the manner in which its results will be reported.
Objectives of supervision that might be considered include the following:
to encourage the TBA to maintain safe and hygienic practices in her work;
to encourage the TBA to refer people to the organized health services for care that she herself is unable to provide;
to help the TBA to solve problems that she encounters in her work;
to encourage the TBA to attend meetings and refresher courses organized for her benefit;
to monitor the activities of the TBA as a basis for evaluating the programme as a whole and the performance of TBAs individually; and
to determine the needs of TBAs in terms of material and other forms of support that they will require for safe practice.

- 31 -
The immediate supervisor of the TBA should be a person who is technically competent in primary health care, including midwifery, and is within reasonable reach of the TBA to be supervised. Depending on the type of staff located at the nearest health agency, this person may be a nurse-midwife, a midwife, a public health nurse, or an auxiliary nurse-midwife. Where such staff are n6t available, it ~ay be necessary to call upon the most capable of the trained TBAs in the community to provide supervision. In the Philippines, a project in which TBAs were used as supervisors of other TBAs- is reported to have "met with considerable success" (see note 30). Where possible, the supervisor should be the person who provided the training for TBAs.
The number of TBAs that one individual can adequately supervise will depend on a number of factors, such as the size of the geographical area to be covered, the accessibility of the villages where the TBAs work, and the other responsibilities the supervisor may have. A supervisor should not have to deal with more TBAs than she can visit regularly, i.e., about once every 4-6 weeks. In addition to the regular visits of the supervisor, an attempt should be made to establish a method whereby TBAs can contact their supervisors more frequently if necessary.
The supervisor should have a clear idea of not only the purpose of her periodic visits to the community - which will be inherent in the objectives established - but also the approach she will use. A visit to the community might include, for example:
(a) a visit to each trained TBA individually, to discuss the work she has done since the last visit (e.g., cases attended and their outcome, individuals referred, and problems encountered); to review her record book; and to replenish her supplies;
(b) a meeting in which all trained TBAs in the community participate and discuss problems they encountered;
(c) a visit to the home of one mother that each of the TBAs has delivered, to discuss the way in which the delivery was conducted, to assess the health status of the mother and infant, and to ascertain the family's level of satisfaction with the TBA's performance;
(d) a discussion with village leaders in order to obtain their opinion of how well the TBAs are performing and the extent to which the community appears to accept the practices of the trained TBAs; and
(e) a discussion with other health workers in the village in order to gauge and help to solve problems arising between them and the trained TBAs.
The plan for supervision should also include arrangements whereby the immediate supervisor of TBAs can report to her senior as regards the results of the supervisory visits. In geographically remote villages, where the immediate supervisor is likely to be a trained TBA from the community, special arrangements for reporting will have to be devised. If the immediate supervisor is to participate in the process of evaluating the TBA's work for a special purpose, e.g., for the renewal of the TBA' s annual permit to practise, she should be aware of the points to be considered in the appraisal and of the form (oral or written) in which her report is to be presented.
In order to ensure that supervision is carried out on a regular basis, the immediate supervisor's functions and specific tasks relating to the supervision of TBAs should be included in her job description, and her performance of these should be monitored by her senior.

- 32 -
Continuing education of the TBA will be provided informally by the supervisor during her periodic rounds, Consideration should be given, however, to a planned programme of continuing education for groups of TBAs. The frequency of group meetings will depend on the ease - or difficulty - of getting people together and may range from once a month to once a year. Such meetings should include a discussion of: the work that the TBAs have done in the interim period; the problems that they have encountered; whether they solved the problems and, if so, how; and their needs, The TBAs should also be apprised of new developments that may affect their work, If TBAs are expected to undertake new tasks, i.e., tasks that their initial training did not take into account, a programme will need to be set up to provide them with the appropriate training,
Sometimes organizational innovation can simplify the task of supervision. In parts of the region of Thies in Senegal, the problem of supervising widely scattered TBAs after training has been partly solved by the establishmen.t of rural maternity centres, These are staffed by TBAs from the area, working in shifts for periods of 48 hours. Each centre is used by women from a number of villages, A professional midwife from a town in the region visits each centre regularly (see note 31). A rather similar project has been in operation in a rural area of Brazil since July 1975 (see note 32),
Other countries have other methods of supervision, In Costa Rica, for example, (see note 33) one of the conditions under which a. TBA is allowed to practise is that the prospective mother must obtain, from the health centre, a permit to have her baby delivered at home by a TBA. A translation of the form used is shown in Fig, 13, Each mother attended by a TBA is supposed to be visited by a nurse or auxiliary nurse, who is required to produce a report on the visit, but the workload. of professional staff often makes such visits impracticable, A nurse-midwife completes a report on each TBA every year. A copy of the form used is shown in Fig. 14. The TBA is required to send a birth notification to the health centre (Fig. 15) and to keep a record of all.her deliveries.
7.3 Supporting services
The supporting services needed to keep the. progranune running smoothly include:
the replenishment of supplies and equipment neede.d by the TBA;
procedures for referrals and the handling of emergencies;
arrangements for transport and communications; and
procedures for the payment of the TBA if she is to. be a paid employee of the health unit of the community.
7.3.1 Supplies and equipment
If TBAs are to app.ly the techniques they have been taught, they will need appropriate supplies and equipment in sufficient amounts. In ·this regard, questions arise as to: what supplies and equipment they will receive upon completion of their training; what additional supplies they will need on a regular basis; who will be responsible for maintaining the stock of supplies and equipment; and who will be responsible for distributing these to TBAs.
In most training programmes offered so far, the TBA has been given a kit, often the UNICEF kit, but in some cases one that wa.s prepared .in the local area. The kit, which is supposed to contain the basic equipment and supplies needed by the TBA, is usually highly regarded by the recipient, who considers it one of ·the rewards of the training programme,

- 33 -
An adequate reserve of supplies and equipment needs to be kept on hand in the local area, for distribution when needed. The most appropriate person to maintain and distribute this reserve would be the immediate supervisor of the TBA, who could take sufficient supplies along with her when she makes her periodic visits. If the TBA works in an area that is within walking distance of the rural (or local) health centre, she could go to the centre for additional supplies as she needs them. It is important that the supervisor keep a check on the supplies that each TBA is using (e.g., the number of cord packs she has tlsed compared with the number of infants she has delivered) in order to gauge the extent to which the TBA is applying the techniques she has been taught,
7.3,2 Referrals and emergencies
Procedures will have to be established with respect to both the referral of patients and the handling of emergencies. In the establishment of such procedures, the advice of village leaders, the TBAs themselves, and the staff of the health agencies concerned should be solicited, At the very least, such persons should be clearly informed of the procedures established,
Depending on the types of service existing and their accessibility to people in the village, the TBA will probably be expected to refer women to the antenatal clinic and postpartum clinic; to refer mothers to the child-care clinic; to assist in gathering children for immunization clinics; to refer eligible individuals or couples to iamily planning services; and to refer to the health centre any patier,t in whom she detects deviations from the normal.
Regarding emergencies, there may be some that the TBA will have been taught to handle on her own, Others will require specialized services that are available only in hospitals, in which case decisions will need to be made as to whom the TBA is to contact, how the contact is to be made, and the method to be used for transporting the patient,
As a part of the referral system, it may be useful to provide TBAs with identity cards that they can give to patients whom they refer to the health unit, These allow a convenient check on the number and types of patients she refers. Some arrangements should also be made for informing the TBA about what has been done for each individual she referred to the health unit or hospital, and what type of follow-up care she should provide when the individual returns to the village. Questions also arise as to what types of referral forms need to be designed and whether or not there is a need for the development of manuals outlining referral procedures, for the benefit of staff in the health agencies,
7.3.3 Transport and communications
Undoubtedly the grea·test problem that will have to be faced throughout the whole programme - from the data-gathering stage onwards - will be the matter of transport and communications. All kinds of administrative procedure can be described on paper as regards the conduct of surveys, training programmes, supervision, referrals, emergencies, and the replenishment of supplies. However, for geographical E.reas that are, for all practical purposes, cut off from health centres, such procedures will remain nothing more than drawingboard fantasies. Some of the questions that planners need to consider with respect _to transport and communications. are presented in note 34,
Transport and communications are important not only in the planning and implementation of the programme for training and articulating TBAs but also in: (a) the evaluation of the performance of TBAs individually and collectively after they return to their work site, and (b) the evaluation of the impact of the trained TBAs' services on the health status of the people they serve.

- 34 -
7.3.4 Payment for services
The matter of payment for the TBA's services should be discussed with village leaders, and their suggestions should be respected as to both the type of payment they feel would be most appropriate and acceptable in the eyes of the TBA and the community and the manner in which the payment is to be made. The type and manner of payment will largely dictate the strength of the link between the TBA and the organized health services as well as the TBA's future relationship with the community. considered include the following:
In this regard, the models that might be
(a) The TBA becomes a regularly paid employee of the health service. In this instance her services are directly linked to the organized health services - the line of authority and the responsibility for supervision are clearly defined. One possible disadvantage of this model, however, is that the TBA may, in her own eyes and in those of the community, be considered a member of the "establishment". This may destroy the trust her clients and other members of the community previously had in her. Government pay could also well lead to other undesirable changes in the social structure of the community. This model would call for close supervision and evaluation of the TBA's work in order to ensure that the TBA is achieving the amount and standard of work implicit in the salary paid her by the government. If the TBA is to be a salaried employee of the government, she will presumably be paid in the same manner as are other personnel working in the organized health service.
(b) The TBA remains a private practitioner, but in a cooperative relationship with the organized health services. According to this model, the TBA would continue to be paid by her clients, but she would receive supervision from the nearest health centre, to which she would be expected to report her activ·i ties and to refer people for services. The disadvantage of this model is that the organized health services would be completely dependent on the TBA's willingness to cooperate, and thus would have little control over her practice. The advantage, on the other hand, would be that the traditional relationship between the TBA and the community would remain intact.
(c) The TBA becomes a part-time employee of the organized health services, which would pay her for certain tasks, e.g., each delivery she attends and/or each client she persuades to adopt family planning. This model would have advantages and disadvantages similar to those in (a), except that the link with the health services would be more tenuous, particularly as regards aspects of the TBA's work that are not paid for by the health services. Under this scheme, the ministry of health would probably determine the amount to be paid for each type of service. The local health
- agency would need to devise a way of checking on the services rendered by the TBA. Her record book, for example, and the number of her identity cards brought in by clients whom she has referred to family planning services, could provide clues in this regard.
7.4 Records and reports
Quantifiable data on maternal and child health and family plahning are vitally important for national health planning and other purposes. The TBA can assist in the gathering of such data. A system whereby she can record and report the data she is expected to gather will need to be developed. In this regard, the following questions arise:
(a) In the case of TBAs who are unable to read or write, what types of data can they be expected to record? The answer is "none", unless they can have the help of someone in the village who can read and write or unless simple forms are designed

- 35 -
and the TBA is taught how to complete them. Exercises in the completion of sample forms should constitute part of the content of the TBA's training.
(b) In the area of maternal and child health and family planning, what types of data are needed that the TBA might be able to record? In this respect, consideration should be given to the types of data needed: for national health planning, for assessing the progress of the TBA programme, for evaluating the activities of the TBA herself, and for evaluating the impact of the TBA's
services on health status.
(c) How will the TBA record the data? Will she be provided with a record book? Will special forms be needed for the recording of certain types of data? In the case of data for national health planning, there should be uniformity in the types of data needed and, hence, in the format whereby the data are recorded. Thus, it may be necessary for that format to be designed initially by the planning group at the national level, tested at the intermediate and local levels, and modified as necessary. Certain types of data may be of interest only to the local health agency, in which case the agency concerned would need to devise its own system of recording and reporting.
(d) How will .data from the TBA's records be gathered? Will her immediate supervisor gather the data when she makes her regular rounds, or will the TBA be expected to bring a record of her work to the health centre?
(e) Does the heal th centre maintain heal th records on individual .patients and/or families? If so, will the TBA have any responsibilities in this regard?
(f) What types of data are other health workers in the locality gathering? It would be important to ensure that data gathering efforts are not duplicated.
If the data are to be used for the purposes lntend~d, every effort should be made to see that the appropriate data are channelled promptly to the people who are planning to use them. Data collection, as an end in itself, is costly and futile. In many instances, data collected in communities are ap~arently meant only for use by the higher echelons of health service administration. Little if any attention has been paid to tbe possibility that the communities them~,elves might benefit from an understanding of the data in terms of what they reflect concerning the problems of the community and the progress being made by the community to solve them. (See also section 7.7 on the maintenance of community interest in the programme through the feedback and interpretation of data.)
7.5 Relationship of TBAs to other health workers
With the proliferation of various categories of worker at the primary-care level, it is essential that there should be a proper division of functions and tasks among them, and that each worker should understand precisely what he is supposed to do, to whom he is to report, and how his work fits in with that of other health and development workers in the community. At the village level there are likely to be, in addition to TBAs, people assisting with health education and with family planning programmes, other primary-care workers, and development workers. At the level of the rural (or local) health centre, there may be midwives, medical and nursing auxiliaries, public health technicians (sanitarians), and laboratory and other technicians. A job description is necessary for each type of worker, and administrative procedures for reporting, referral, supervision, and team work (including team leadership) must be clearly defined.

- 36 -
7.6 Regulation of the TBA's practice
An important question that needs to be answered in countries undertaking the training of TBAs is how their practice can be regulated, Since the activities of TBAs have been generally sanctioned by customs and rituals that form a part of community life, the arbitrary introduction of legal measures to regulate their practice might well provoke the community's hostility or in some other way disturb the relationship between the TBA and the community.
While it is essential that the public should be protected from unsafe practices on the part of health workers, the best way to ensure such protection in the case of TBAs is difficult to determine. If legislation is to be adopted, it should be preceded by making the people aware of the importance of such control, so that they themselves will demand safe practices. At the same time, it should be borne in mind that, owing to the limitations of the TBA and the cultural, economic, and.geographical factors impinging on her work, it might be difficult to determine where justice lies in cases where a complaint of malpractice arises. Moreover, legislation automatically implies the need for personnel to follow closely the activities of the TBA in order to ascertain whether or not she is complying with the law. It also implies that the means for safe practice are available to the TBA and to the community, which is hardly the case in conditions of extreme poverty.
In the long run, supervision and continuing education may be the best approach to ensuring safe practice by the TBA. Additionally, her acknowledgement by community leaders and clients, and her knowledge that a record is being kept of her activities may go a long way towards making the TBA aware that people are interested in her and in what she is doing and that she must try to fulfil their expectations. A further incentive might be the granting of a certificate indicating that she has successfully completed the necessary training and is thus qualified to practise. This might serve as a temporary permit or licence, to be renewed periodically on evidence of satisfactory practice. The renewal of such a permit would imply the need for: a form of licensing authority; a registry for keeping an up-to-date record of all TBAs in the country; a list of standards for the TBA's practice; and, of course, a system for monitoring the activities of TBAs.
The question also arises as to how TBAs who, for one reason or another, do not undergo training will be treated. In other words, ~f legislation ~s-adopted to the effect that only TBAs who have undergone the necessary xraining and meet certain other specified conditions will be authorized to practise, would the government prosecute untrained TBAs who continue to practise? For both practical and s.ociaL reasons it may be unwise to adopt stringent legislation aimed at putting the untrained TBA out of practice. With the greater satisfaction that clients may derive from the safer practices of trained TBAs, the demand for untrained TBAs is bound to decline, in which case they will either cease practising or undertake the necessary training.
It was mentioned earlier, in the discussion concerning the initial inventory of TBAs, that a permanent register of all TBAs in the country should be kept at the national level. The logistics of keeping such a register up to date will have to be considered. Since the local health agency will, in any case, need to keep an up-to-date record of all TBAs in the area, a system of registration should be instituted at that level, the initial inventory serving as the basis. to register each year.
All TBAs in the area, whether trained or untrained, should be invited The types of data noted in the register should be similar to those
called for in the inventory, the registration form allowing sufficient space for updating and for particular observations. Special efforts will need to be made to keep track of untrained TBAs, both those listed in the initial inventory and those beginning practice,
The register will not only provide a measure of control but also reference for the mobilization of suitable personnel for other health activities. It will also make it possible to determine the attrition
serve as a convenient and development rate of TBAs and changes

- 37 -
in their characteristics~ such data being useful for the planning of future training and refresher courses and for health manpower planning in general. Registration data obtained at the peripheral level will need to be relayed to the intermediate level and from there to the central agency charged with keeping the national register. The card used for the
. registration of TBAs. in the Philippines is reproduced in Fig. 16. Perhaps one shortcoming of the card is that it lacks sufficient space for the updating of information and for additional observations.
7.7 Maintenance of interest in the programme
Once the enthusiasm generated by the training programme is over, and unless constant surveillance is maintained, there is likely to be a general tendency on the part of TBAs, the staff of the health agencies, and the people in the community to settle back into their old ways of doing things. Responsibility for the follow-up of the programme begins with the individual (or group) designated at national level to plan and implement the programme. Continuous surveillance at the provincial and district levels is part of that responsibility, and methods for such surveillance should be built into the plan for programme implementation. It is essential that, at each of these levels, a person be assigned responsibility for programme implementation. The names and location of such persons should be kept on file at the office of the person responsible at the national level, and a system of communication between levels. should be devised.
Personnel in health agencies change frequently. New people are added to the staff, transfers are made, and.people are promoted, retire or resign. For those who remain, priorities are constantly shifting, so that the TBA programme that was initiated with enthusiasm tends to be neglected. Senior persons at national and provincial levels can help to maintain motivation at other levels through periodiq visits to health agencies, requests for reports, and the feedback of information on the progress of the programme. Feedback might take the form of:
(a) a regular issue of progress summaries to health units, designed to enable the health unit to compare its own performance with. that of similar units and to analyse factors contributing to or retarding progress;
(b) oral reports to TBAs and to community leaders (by either the supervisor or more senior personnel from the health agencies) regarding progress in the area and the progress of the programme as a whole; and
(c) publicity through articles in national and local newspapers, radio, and television.
PROGRAMME EVALUATION
Programme evaluation is essentially the process of determining the extent to which predetermined objectives have been attained. The methods of evaluation described in section 6 were limited to those that could be used, during and as a part of the training course, to assess the extent to which the trainees attained the learning objectives specified. The methods described hereafter are those that aim at an assessment of:
(a) the achievement of the training programme in terms of the .number of TBAs enrolled and the numbers successfully completing the training;
( b) the performance of trained. TBAs in the communities they serve. in terms .of the quantity and quality of service.s they provide; and
(c) the impact of the services provided by trained TBAs on the health status of the populations they serve.

- 38 -
For each of the above-mentioned assessments it is necessary to have information that will allow a comparison of the respective factors concerned at two points in time, i.e., at a point prior to the start of the training programme (baseline data) and at the point when the evaluation is being undertaken, which, in the case of (b) and (c) above, should be no less than a year after the TBAs concerned have completed the training course, and periodically thereafter. Where baseline data are not available, and even where they are available, an alternative is the comparison of the performance and impact of trained TBAs with that of untrained TBAs and that of other health workers.
8.1 Assessment of the training programme
Assessment of the training programme in terms of the number of TBAs enrolled and the number completing the programme is a fairly simple procedure. The only baseline information needed is the number of untrained TBAs existing in the area concerned prior to the start of the programme. The inventory of TBAs described earlier should provide this information. The numbers enrolled in the training programme, as well as the numbers completing it, should form a part of the records kept by the administrator of the programme.
Comparisons, in both absolute and proportional terms, can be made with respect to:
(a) the number enrolled in the programme versus the number of those untrained prior to the programme;
(b) the number successfully completing the programme versus the number enrolled; and
(c) the number successfully completing the programme versus the number of those untrained prior to the programme.
If one of the broad objectives of the training programme is to provide training for all untrained TBAs in a defined area, the comparisons mentioned above will show the progress made toward the achievement of this objective.
8.2 Assessment of the performance of trained TBAs
The performance of trained TBAs can be assessed in terms of the quality of their work and the amount uf services they provide. With respect to quality, the primary objective would be to determine the extent to which the trained TBAs are applying the safe methods of practice taught them during the training programme. With respect to quantity, the primary objective would be to ascertain the extent of the increase in the numbers of mothers and chi~dren receiving specified services direct from the TBAs concerned or as a result of referrals by them. Each of these aspects of evaluation is dealt with below.
8.2.1 Assessment of quality of services
High scores on tests of individual performance administered during the training programme do not necessarily mean that the TBA will apply what she has been taught once she completes the programme. This may be so for several reasons, one of which might be that the training programme failed to persuade the TBA that certain practices are really worth applying. She may even believe that some of them are hazardous. For example, when answering test questions or when practising under supervision, she may behave in a way that indicates she has understood the importance of using a clean instrument to cut the cord or of referring to the health centre persons whose health problems she cannot handle. Privately, she may think that the importance of cleanliness is exaggerated by professionals and that the appropriate response to complications is prayer rather than referral.

- 39 -
A related problem is that ideas about acceptable practice form part of the culture of the community in which the TBA works. Some safe practices advocated by staff of the organized health services may be culturally alien to the community and, in communities that have not been adequately prepared beforehand, the TBA who tries to apply such practices may find herself less respected than she was previously. For example, a refusal to massage the mother's abdomen during a late stage of labour might be construed as a dereliction of duty in areas where the provision of this kind of massage is a well-established custom. Even where both the TBA and the community are convinced of the value of such practices, there may be other barriers to their implementation. For example, the absence of clean water and limited referral facilities may seriously impede the TBA's ability to perform as she was taught.
Direct observation of the TBA's methods of practice is perhaps the best way of assessing the quality of her practice. Even this method, however, has its limitations in that, while a TBA may perform as she thinks the supervisor (observer) expects her to, she may perform otherwise in the absence of the supervisor. Direct observation, if it is to be an effective tool in evaluation, should be more than just a once-and-for-all event.
The immediate supervisor (or other person doing the assessment) should periodically accompany the TBA on her rounds to see how she cares for women at various stages of the maternity cycle (before, during, and after birth). Moreover, evaluation of the TBA's quality of practice can be enhanced if, in addition to direct observation, the supervisor interviews several of the TBA's clients in order to obtain information on the type of advice the TBA has given them with respect to, for example, nutrition, infant feeding, and family planning, and the manner in which she dealt with, for example, the newborn baby's umbilical cord.
In Ghana an attempt was made to assess the quality of practice of trained TBAs by a rather indirect method, which was exceptionally revealing. According to the report of that assessment (see note 35), 2 trainers and 38 of 42 trained TBAs were interviewed in order to assess, inter alia, the extent of field supervision received by the TBAs, the TBAs' experiences in the community, and the usefulness of the UNICEF kit in the field. With respect to the kit, particularly, interesting and important observations may be found in the report. A few of these, which are presented in note 35, show the contradictions between what some TBAs aver by word and what they do in practice. They also point to the importance that trainers should attach to the need for TBAs to have repeated practical training in the use of each item in the kit.
8.2.2 Assessment of quantity of services
If one of the objectives of a programme for training and using TBAs is to improve coverage of the population with services in maternal and child care and family planning, the performance of TBAs may be evaluated by seeking answers to such broad questions as the following:
(a) Are proportionately more women receiving prenatal and postnatal care than was the case before the training programme for TBAs was started? If so, to what extent is this attributable to trained TBAs as opposed to untrained TBAs and to staff of health agencies?
(b) Are proportionately more deliveries being attended by trained than by untrained TBAs? This question may also be expressed in terms siailar .to those in (a) above.
(c) Are more people in the village accepting or continuing modern family planning methods? To what extent is this attributable to trained TBAs?
(d) Is more frequent use being made. of the services provided by the centrally organized health agencies? To what extent is this attributable to trained TBAs?

- 40 -
Again, in order to answer such questions, it will be necessary to have information that will allow a comparison of the factors concerned at two points in time, e.g., at a point prior to the start of the training programme for TBAs and at the point when the evaluation is being undertaken. Unless the baseline data are available, evaluation in the above-mentioned context will not be not be possible. (Again, however, a~ alternative is the comparison between trained TBAs and others at one or more points in time after the trained TBAs have resumed practice.) As regards the trained TBA, four basic methods may be used to obtain relevant data: direct observation of the work of the TBA; discussions with the TBA's clients and others in the community about the TBA's work; the use of information from records and reports; and discussions with or questionnaires to health agency personnel involved in the work of TBAs.
In a search through the literature, the only examples found of evaluation of the TBA's performance over time were in respect of her work in recruiting clients for family planning clinics. No reports were found of improvement (or deterioration) in her performance in attending births or in referring people to health clinics for such .services as antenatal care. On the other hand, there are a number of reports of surveys of the post-training performance of TBAs. For example, in Bolivia data were collected on the number of births attended and referrals made by trained TBAs (see note 36). In Mexico, as a second example, data were collected on a wide range of services provided by trained TBAs (see note 37).
According to some trainers of TBAs, in areas where health facilities are very limited, one result of the training of TBAs is that existing facilities have been overwhelmed by the number of pregnant women referred. In such circumstances, it would be important to determine what proportion of the referrals reflects the ability of TBAs to j_dentify and refer high-risk patients, as opposed to patients requiring routine care. The feasibility of doing so is implied by the results of a study in Dar-es-Salaam (see note 38). A recent WHO publication provides a general introduction to the use of risk factors as a means of making optimum use of limited resources for maternal and child care (see note 39).
Perhaps most of the evidence available for measuring the performance of the TBA concerns her performance as a family planning worker. In this regard, the most common method cif evaluation (after a training programme) has been to record the number of women accompanied or referred by TBAs to a health centre for family planning services or to ascertain what proportion of those who adopted family planning were motivated by TBAs. This type of assessment, if extended over a long enough period of time with respect to a specific area, seems.very likely to result in disappointment with the TBA's performance. It seems to be a common experience that performance in this respect declines over time. The decline, according to some authors (see note 40), is attributable to various factors, the main one being that the recruitment of adopters of family planning slows down when the most receptive persons in a local population have been recruited.
In an experimental programme in Central Java, an attempt was made to measure the exterit to which TBAs (known there as "dukuns'') advised their clients to visit the family planning clinic. The form used for the purpose is shown in Fig. 17. An explicit purpose of the procedure was to remind the TBA to encourage mothers to visit the family planning clinic.
In most countries, the TBA has not been expected to do more than encourage local women to use the family planning service. Some attempts have been made, however, to use and evaluate her as a distributor of oral contraceptives. The rate at which clients recruited by TBAs continue to use oral contraceptives is one of the measures used to evaluate TBAs in Malaysia (see note 42).
Whether the objective of a family planning programme is to lower fertility or to contribute to maternal and child health, the programme will normally be directed towards reducing typical family size by increasing the interval between births. It follows, therefore,

- 41 -
that one important aspect of the TBA's performance is her ability to recruit clients with relatively small families. In an experimental programme in Central Java, clinic record cards for women recruited by TBAs during a specified period were examined in order to assess the TBAs' performance with respect to family size and other characteristics of the women recruited (see note 43).
8.3 Assessment of impact on health status
While improvements in the health of mothers and children should be the primary objective of any training programme for TBAs, the respects in which and the extent to which this objective is achieved are very difficult to evaluate. Because health is affected by a constellation of factors, of which the practices (good or bad) of the TBA are only one, it would usually need studies beyond the range of local resources to determine the effect of a change in her practices on characteristics of health status. In areas where, in addition to TBA training, efforts are also being made to improve such health-related factors as nutrition, housing, education, environmental sanitation, and transportation, improvements in health are likely to be due to a combination of these factors. Conversely, where malnutrition and a poor environment are the major causes of excessive mortality and morbidity, even the best trained TBAs may be unable to have much effect on the health of the populations they serve.
A connnon response to the difficulties of measuring impact is to make no attempt to assess it but simply to assume that training will have the desired outcomes. This assumption is more plausible when the TBA's work is subject to continuing supervision (see section 8.2.1) than when, as is more connnon, the limited availability of professional personnel and other resources
makes effective supervision impracticable.
Sometimes it may be possible to assess the impact of training by analysing trends in such indicators as neonatal mortality rates by cause and by type of birth attendant. Usually, however, the necessary data are not available. Where they are available, trends in the performance of TBAs can be compared with trends in the performance of other workers, and with the performance of TBAs in other areas. Another possibility is to undertake periodic surveys of the kind described in section 4.3.3 and Note 13. Frequently it may not be feasible to do more than use records of such activities as the referral of difficult cases to the health centre by trained TBAs, as a means of assessing their contribution to better health care.
Owing to the difficulties mentioned above, it is impractical to offer very precise guidance on methods of assessing impact. While some possibilities are suggested, most of what follows is directed towards emphasizing the importance of basing programmes on a realistic appraisal of their potential impact and of doing what is feasible to assess their actual impact. It should always be borne in mind that a well trained TBA will often be in a position to alleviate pain and distress. Her capacity to do so is of first importance whether or not it can be measured.
8.3.1 Maternal mortality
Maternal mortality (i.e., mortality ascribed to childbirth and the puerperium) seems to be one of the more obvious choices among possible indicators of the quality of midwifery practice. In fact, while maternal mortality may be of some value as an indicator of broad national trends, it is of little use in measuring the success of a TBA programme. The main reason for this is that maternal deaths are relatively infrequent events, even when the rate is quite high. A high rate of 5.0 maternal deaths per 1000 livebirths would mean only one maternal death every few years in a typical Asian or African village. For a reference on recent trends in maternal mortality in various countries, see note 44.
The use of the maternal mortality rate as an indicator of broad trends and as a possible, although perhaps doubtful, measure of the success of a midwife training programme is described in a report on the training and activity of village midwives in the Sudan (see note 45).

- 42 -
Two special inquiries into maternal mortality in rural Bangladesh are revealing about the nature of the problem and about the impracticability of using maternal mortality, however accurately measured, as a specific indicator of the impact of a TBA programme. While none of the deliveries investigated was conducted by a trained TBA, the results of the studies suggest that some causes of maternal mortality, such as postpartum tetanus, could be prevented by simple cleanliness in the management of childbirth - a preventive measure on which TBA training should strongly focus. The authors of the report on these studies state, however, that at least one-third of maternal deaths were due to complications of pregnancy requiring facilities for anaesthesia, surgery, and blood transfusion. Where such facilities are not available, neither TBAs nor any other health personnel can prevent mortality in the case of patients for whom such facilities are mandatory. (See note 46 for other relevant observations.)
8.3.2 Infant mortality
The author of a recent report on world trends in infant mortality (see note 47) states that between 10 and 12 million of the 125 million children born in 1975 were destined to die before reaching their first birthday. He points out that the chance of surviving the first year is one of the clearest indicators of social and economic development. In tropical Africa about 1 child in 5 dies during the first year. In Scandinavia, it is 1 child in 100. The author divides the less developed regions into three categories according to their level of infant mortality: 65-100 infant deaths per 1000 births in Latin America and eastern Asia except Japan; around 140.in northern Africa, south Asia, and Melanesia; and about 200 in tropical Africa.
In developing countries, 60-80% of all infant deaths occur in the post-neonatal period, but deaths in the neonatal period are a more sensitive indicator of the quality of obstetric care and of the scope for its improvement through the use of trained TBAs.
A major contribution to knowledge of the factors contributing to neonatal mortality was part of the yield of the Inter-American Investigation of Mortality in Childhood. It is clear from the findings of that study that, in a substantial proportion of child deaths, the underlying cause of death is one over which TBAs would be powerless. Indeed, even modern health services were apparently powerless to prevent death in most such cases. This is borne out by the study's finding that 67% of the children who died during the neonatal period had been born in hospital and had died there. A further 18.5% had received treatment in hospital for what later proved to be the underlying cause of death. The role of low birth-weight, immaturity, and nutritional deficiency as correlates of neonatal death is revealed by the study's findings (see note 48).
The problems of relating training to impact were well brought out in a study of midwifery practices in rural Punjab (see note 49). The purpose of the study was to identify specific factors in the clinical course of parturition contributing to infant deaths and to determine differences in methods employed by trained and untrained midwives in explanation of the higher death rates among infants delivered by the untrained. An analysis of neonatal deaths in relation to the instrument used for cutting the umbilical cord showed that such deaths were lowest, and that there were no cases of tetanus when a knife was used.
8.4 Conclusions
The preceding paragraphs and related notes clearly suggest that the measurement of the TBA's impact on health status is no easy matter. Equally clear is the fact that, if decisions to train and use TBAs are based on the hypothesis that trained TBAs will bring about an improvement in the health status of mothers .and children, then serious efforts should be made to test that hypothesis in ways that are more meaningful than most of those used so far. Perhaps the greatest benefit derived from the evaluations attempted thus far has been that they point to the need for more adequate instruments for measuring impact.

- 43 -
Regarding evaluation of the TBA's performance, as discussed in section 8,2, this should not be confused with evaluation of impact on health status, Although it would appear that the studies cited in that section were intended specifically to evaluate performance, most of them did not include comparisons between two points in time or betweeh trained TBAs, untrained TBAs, and the staff of organized health services,
The kinds of data that might possibly provide measures of both the performance of trained TBAs (as discussed in section 8.2) and the impact of trained TBAs (as discussed in section 8,3) are listed in Fig, 18, Unfortunately, much of the information required is least likely to be available in areas where the TBA is the predominant source of midwifery practice. Where this is the case, crude approximations for a number of the measures involved may suffice for the time being. However, for really meaningful evaluation and further decision-making and planning with respect to the training and use of TBAs, more solid data on a variety of factors are essential. For example, a small study in Indonesia of 44 neonates admitted to hospital with tetanus neonatorum found that 40 of the births had been attended by TBAs and that, of these TBAs, over half ("at least 23") appeared to have been trained, i.e., they possessed a UNICEF kit (sec note 50), Such a finding might lead to the assumption that there is no point in spending time and money on the training of TBAs. In cases such as that one, it would be essential to have more precise information on the various possible factors involved, some or all of which may have had little to do with the TBA's behaviour.
As suggested earlier, TBAs can be an important source of various types of information needed for evaluation and planning, Every effort should be made to train them to report on matters that lie within their competence to observe and judge. For example, they might be trained to report deaths,indicating what they think is the cause. Most trained TBAs will have learned to recognise at least tetanus and diarrhoeal disease as possible causes of death. In all cases, the TBA needs to be taught how to ir1form the heal th centre about: the deliveries she attends and the results; other health activities in which she participates; and individual and community health problems, Furthermore, other members of the community,
particularly the women, may, if properly approached, be an invaluable source of information. Well-designed periodic surveys of community members should therefore be organized to supplement information derived from TBAs. Additionally, a well-developed system of data recording at each health establishment is, of course, mandatory for both the evaluation of the performance of TBAs individually and collectively and the evaluation of their collective impact on health status.


- 45 -
F I G U R E S

Fig. 1. Tasks from among which those authorized for undertaking by the trained TBA might be selected
Fig. 2. Questionnaire used in national survey of hilots (TBAs) in the Philippines
Fig. 3. Questionnaire prepared for a survey of the knowledge and practice of hilots (TBAs) in the Philippines
Fig. 4. Translation of questionnaire used for a survey of the knowledge and practice of TBAs in a rural area of Mexico
Fig. 5. Translation of a questionnaire used for an enquiry among women, many of whom were clients of TBAs, in a rural area of Mexico
Fig. 6. Some existing practices among TBAs and proposals for their modification, as seen by a group of public health nurses
Fig. 7. Example of a learning module
Fig. 8. Sample checklist to assess a TBA's performance during a delivery demonstration in the home
Fig. 9. Sample checklist to assess the use and care of the delivery kit or bag by trained TBAs
- 46 -
LIST OF FIGCRES
Fig. 10. Translation of a test used in a TBA training programme in ,iexico
Fig. 11. Page from an illustrated manual for TBAs in the Philippines
Fig. 12. Illustration from a WHO manual for the training of primary health care workers
Fig. 13. Translation of form used in Costa Rica to authorize birth attendance by a TBA
Fig. 14. Translation of form used in Costa Rica for making an annual report on a TBA
Fig. 15. Translation of form used by the TBA in Costa Rica to notify the health centre of a birth
Fig. 16. Front and back of a form used for the registration of the TBA in the Philippines
Fig. 17. Form used in a programme in Central Java to record the dukun's (TBA's) reported efforts to encourage her clients to visit a family planning clinic
Fig. 18. Some likely indicators of the quantity of services provided by TBAs and the impact of such services on the health status of mothers and children

- 47 -
Fig. 1. Tasks from among which those authorized for undertaking by the trained TBA might be selected
Antenatal care
1. Identification of pregnancy and perception of abnormal progress.
2. Provision of advice to pregnant women about diet and the preparation and
preservation of food.
3. Provision of advice to pregnant women about personal and domestic hygiene and the importance of rest and sleep.
4. Provision of advice to pregnant women about antenatal services available and the importance of using them.
5. Identification of the canmon discomforts of pregnancy and the provision of treatment for them or referral for treatment by the health service when discomfort is severe.
6. Identification of risk factors and danger signs; referral of women at risk to health services; and follow-up care.
7. Referral of apparently normal pregnant women to the health service for routine antenatal checks and services.
Delivery
8. Identification of the approach of labour ..
9. Management of apparently normal labour.
10. Management of normal delivery.
11. Management of separation and expulsion of the placenta.
12. Identification of abnormal circumstances during labour or delivery; the provision of emergency treatment; and referral to health service.
Care of newborn
13. Provision of care to the newborn, including attention to breathing, cord care, and the environment.
14. Identification of deviations from the normal in the newborn and provision of treatment or referral to the health service.
15. Provision of assistance to the mother with the initiation of the motherinfant relationship, including the commencement of breast feeding.
Postpartum care
16. Identification of normal changes in the uterus, abdomen, and breasts during the puerperium.
17. Management of breast~feeding.
18. Identification, treatment, and referral of complications affecting mother or baby during the postpartum period.
19. Provision of advice to the mother about personal hygiene and the importance of an adequate diet, prolonged breast-feeding, and appropriate exercises.
20. Provision of advice to the mother about the resumption of sexual intercourse and menstruation, and the implications of these for the_ possibility of conception.

- 48 -
Fig. 1. (Continuation)
Infant care
21. Identification of circumstances detrimental to the welfare of infants, and the provision of advice on this subject to parents.
22. Identification of deviations from the normal in the progress of infancy, and referral of cases to the health service,
23. Identification of common infections and disorders of childhood, provision of treatment, referral of cases to the health service, and provision of follow-up care.
24. Provision of advice to the mother about infant care throughout the first year of life, including advice on immunizations, periodic examinations of apparently well infants at a clinic, infant diet, cleanliness of the infant, hygienic measures for the prevention and control of communicable diseases, and simple first aid.
25. Encouragement of mothers to participate in classes on infant health care organized by the health service.
Family planning
26. Identification of circumstances indicating that it is in the interests of the family to delay a further conception.
27. Provision of advice to mothers or couples about the merits of spacing pregnancies and about methods of contraception and sources of supply of contraceptives,
28. Referral of mothers to family planning clinics.
29. Supply or re-supply of contraceptives to couples.
30. Provision of advice to couples about side-effects of contraceptives.
31. Referral to the health service of couples seeking advice on infertility.
Public health duties
32. Participation in public health schemes.
33. Reporting of births and infant deaths for registration, or persuasion of parents to do so,
Source: Derived from a more detailed list presented in the publication cited in note 1.

- 49 -
Fig. 2. Questionnaire used in national survey of hilots (TBAs) in the Philippines
Bureau of Health and Medical Services DIVISION OF MATERNAL & CHILD HEALTH
Province City ~------~---~-~-Muni c i pa U t y Barr{o ( or P-6-b~l_a_c_i_o_n_) ______ _
HILOT MANPOwER STUDY
RHU Puericulture Center Health Center
Check
§ -------------------------------------------------------------------------------------------- -
Name: (First) (Middle)
Nickname:
(Surname)
Address: -----~ ----------~---~-~-~-~-~--~-~-~--1
Civil 8tatus: Single D Married D Separated D Widow/er
Female
D D Age (last birthday) yrs. Sex: Male O
1)
2)
3)
Literacy
Cannot read nor write Can read, cannot write Can read and write Can write name only
Schooling
None at all Grade 1 - 3 Grade 4 - 6/7 High School 1 - 2 High School 3 - 4 College 1 - 3 College 4+
Years in P1'actice
--------
4) Training Deparbnent of Health/UNICEF Training Institute of Maternal and Child Health>-Puericulture Center Personnel
->----
Kin (mother~ grandmother~ etc.) Private Physician Private Nurse/Midwife Missionary Self Others (specify)
>----
-
5) Activity Status in l9?2 No practice at all § Partially practiced (1-11 months) Fully practiced (all 12 months)
6) Number of Deliveries in l9?2: ------------------------------------------------------------------------------------------------ --------------------------------------------------------------------------------------------
Signature of Data Collector Designation: Nurse[] Midwife O Attested by:
Signature of Supervisor
Signature of Hilot or
Thumbmark of Hilot
= =============--=--=-----======--====================================--=---=---=--===--=---== INSTRUCTIONS
Items 1 and 2 - Check rhe appropriate box Item 3 State total number of years in practice in the municipality
Item 4 Item 5 Item 6
and/or other municipalities - Check appropriate box - Check appropriate box - Count and state only the deliveries assisted between January-
December l9?2; do not count deliveries in l9?3 nor deliveries ~n l9?l or previous years
Identity of Hilot: If hilot can sign her name let her affix her signature in blank provided for. If illiterate, take thumbmark. Submit accomplished foY'l'TI to your city/provincial nurse supeY'Visor.
Source: See note 6

Fig. 3.
- 50 -
Questionnaire prepared for a survey of the knowledge and practice of hilots (TBAs) in the Philippines
ASSESSMENT OF HILOT TEACHING EILOT I s QUESTIONNAIRE Study of Traditional Birth /;:ttenciar:ts, Phase II ~
B f H 1th d Md" 1 ~ • ~orm No. 2.1 W'eau o ea,, an e -z..ca" cer;J1,'.'.!es
=_QiQi~ion=QL Maternal_and_Chila Eea:t~================5
·=·=========--===--------------
I. IDENTIFYING DATA OF HILOT:
NAME: (Family) (Given)
II. UTILIZATION OF HILOT:
1. Do you usually see/visit your patients during their pregnancy?
(CODES) i
(Do not fill) 1.
012~ 03~ D SOMETIMES
1.la If YES or SOMETIMES, at what month of the pregnancy do you usually start seeing them?
(Encircle only one)
1 2 3 4 5 6 7 8 9
1.1b If YES or SOMETIMES, at what month should pregnant women be seen or visited by you? (Encircle only one)
1 2 3 4 5 6 7 8 9
1.lc If YES, how often do you usually see the woman during the whole period of pregnancy?
III.PREGNANCY:
1-3 TIMES 4-6 TIMES 7-9 TIMES MORE THAN 10 TIMES
1.2a If NO, why not (Check only one)
1.1 a 1.1
NOT NECESSARY 1.1 1.2 1.2 NO TIME, TOO BUSY
RESIDENCE TOO FAR REFERRED TO HEALTH CENTER OR PRIVATE CLINIC
Os ______ _
b-c --a --b
1.2b If NO, when do you usually see your patients? (Check only one)
~ 1 WHEN PATIENT HAS COMPLAINTS 2 START OF LABOR 3 AFTER DELIVERY ONLY 4 --------~
2. What changes -z..n the woman would make you suspect that she is pregnant? 2.
~ 1 STOPPING OF MENSES 2 NAUSEA, VOMITING 3 ABDOMINAL ENLARGEMENT
· 4 WIDENING OF HIPS 5 DARKENING OF NIPPLES ~
6 BREAST ENLARGEMENT 7 DIZZINESS, HEADACHE 8 PULSATION IN THROAT 9 CHANGE IN APPETITE/MOOD
10 ___ _
3. Below is a drawing of the i~jerr.al reproductive organs of women. 3. Identify the numbered str~'.]tc<I'es.
~ 1 NO STRUCTURE T;JEI,"!' I? IZD 2 ONE STRUCTURE IDENTI?I~D 3 TWO STRUCTURES 4 THREE STRUCTrnES 5 FOUR STRUCTURES
4

- 51 -
Fig. 3 (Continuation)
4. Should a pregnant woman eat certain foods believed good for her and 4. her baby? D 1 YES O 3 I DON'T KNOW D 2 NO D 4 AM NOT SURE
4.1 If YES, what foods should be eaten by pregnant women and what is 4.1 the purpose of each?
Food to Eat
4.2 If NO, why not?
D 1 NOT IMPORTANT D 2 I DON'T KNOW
Purpose
B ! ALL FOODS ARE NECESSARY
5. Should pregnant women avoid eating certain food believed bad for them and for their babies? [3 ~ !~s B ! ALL FOODS ARE NECESSARY
4.2
5.1 If YES, what are these foods to be avoided and for what reason? 5.1
Foods to be Avoided Reason
5.2 If NO, why not?
0 1 NOT IMPORTANT 0 2 I DON'T KNOW
B ! ALL FOODS ARE GOOD
6. Is there a need to massa8e or manipulate the abdomen of a woman during pregnancy?
B 1 YES 2 NO
SOMETIMES I DON'T KNOW
6.1 If YES, for what purpose? (Check only one)
~ 1 TO SOFTEN MUSCLES AND UTERUS IN ORDER TO EASE DELIVERY 2 TO PUSH UP ABDOMEN 3 TO BRING DOWN BABY NEAR PELVIC OUTLET 4 TO CORRECT ABNORMAL FETAL POSITION 5 ~~~~~~~~~~~~~~~~-
6. 2 If NO, why not? (Check only one)
§ 1 I DON'T KNOW HOW 2 NOT NECESSARY ! DANGEROUS TO MOTHER/BABY
5.2
6.
6.1
6.2

- 52 -
Fig, 3. (Continuation)
7. Do pregnant women nee:i t:J :::1.-:e by "'.:Jutr. or herb preparations be Ueved {!:J x:. -,::Jr S,e"'. ar,.i f"cJ2· t\eir bc:.::;ies?
D 1 YES 0 2 NO
7.
7.1 If YES, what are ~nese mec:.~c&ne or herbs and for what purpose? 7.1
Medicine/herbs Purpose
7.2 If NO, why not? (Check only one) 7.2
~ 1 I DON'T KnOW OF ANY HERB OR MEDICINE 2 NOT NECESSARY 3 DANGEROUS TO MOTHER/BABY 4 ~~~~~~~~~~~~~-
8. What do you think are the danger signals to watch for in pregnant 8. women that indicate that something is wrong with the pregnancy?
~ 41!
5
ABDOMINAL PAIN ~ 6 SWELLING (face, arm, legs) BLURRING 7 HEADACHE CONVULSIONS 8 DIZZINESS FEVER WITH CHILLS 9 VAGINAL BLEEDING PERSISTENT VOMITING 10 VARICOSITIES
9. If a p1'egnant woman develops swelling of the face, arms, or legs 9. what could be the cause of the swelling? (Check only one)
§ 1 TOO MUCH SLEEP D 4 DON'T KNOW 2 EVIL SPIRITS [J 5 WATER RETENTION WITH SALT 3 BERI-BERI INTAKE
10. What do you think should a pregnant woman do to avoid developing 10. swelling?
~ 1 A VOID OVER-SLEEPING ~ 5 AVOID OVERvlEIGHT 2 APPEASE EVIL SPIRITS 6. REGULATE SALT INTAKE 3 WEAR AMULETS 7 EXERCISE 4 I DON'T KnOW 8
~~~~~~~~~
11. Have you seen or knoum some women who had convulsions during 11. pregnancy, delivery, or just after delivery?
0 1 YES O 3 I DON'T REMEMBER [J 2 NO [J 4 A!1 llOT SURE
12. Why do you think some "'':;,:::er. n:oe con:iu 7,sions d:uring pregnancy or 12. delivery?
~ 1 NORMAi,, p;,2T (jf ::-_-.::.J,,.c.._,,:;~ ~ ;:; ."c:~:;,"· BLOOD PRESSURE 2 EVIL SPIRBS :J :::':::z::;..sIGET 3 HEREDTTAHY 7 ?':;':'.'~ O? SALTY FOOD 4 FATIGUE

- 53 -
Fig. 3 (Continuation)
13. What steps were taken or what would you do if a pregnant or just 13. delivered woman developed convulsions?
§ 1 CALL FOR FAITH HEALER § 4 MASSAGE 2 LEAVE ALONE . . 5 REFER TO HOSPITAL, CENTER 3 GIVE MEDICINE, HERBS 6 --------------------~ IV. LABOR
14. When you are called to assist a delivery, what do you usually bring 14. with you that would be needed in your assistance of the delivery?
1 ALCOHOL 2 AMMONIA 3 ANTISEPTIC SOLUTION 4 APRON 5 COTTON· 6 CORD DRESSING/GAUZE 7 ERGOTRATE 8 FORCEPS
9 GLOVES 10 NOTEBOOK 11 OIL 12 PITOCIN 13 POWDER 14 TOOL FOR CUTTING CORD 15 VITAMINS
15. Do you usually give the women in labor some medicines/herbs/food to relieve pain or to hasten delivery?
fJ 1 YES, FREQUENTLY D 3 NO, NEVER D 2 YES, SOMETIMES
1 2 3 4 5 6 7 8
15.
15.1 If YES, or sometimes, what are these medicines, herbs, or food 15.1 that are given and what is the effect of each?
16.
17.
Medicines/herbs/foods Effect
15.2 If NO, why not? (Check only one)
§ 1 I DON'T KNOW OF ANY 2 NOT NECESSARY, WOMAN WILL BE DELIVERED ANYWAY 3 NO AUTHORITY 4 --------------------------~
What procedures or practices do
the §babr NONE . 2 LET MOTHER WALK 3 OPEN WINDOWS, DOORS 4 LET MOTHER JUMP
While the woman is in labor do by inserting your fiYigers into n 1 YES, FREQUENI'LY
D 2 YES, SOMETIMES
17.1 If YES, for what purpose?
you observe to hasten the birth of
§ 5 PUSH DOWN ABDOMEN (SALAG) 6 APPLY OIL, HERBS IN VAGINA 7 PINCH BAG OF WATER 8 ----------------------~
you usually examine her internally the birth canal?
D 3 NO, NEVER
1 DETERMINE DILATATION, EFFACEMENT 2 FOLLOW WHAT OTHER HILOTS ARE DOING 3 DEMONSTRATE COMPETENCE TO PATIENT 4 GUIDE BABY'S HEAD 5 MAKE BIRTH CANAL BIGGER 6 ---------------------
15.2
16.
17.
17 .1
9 10 11 12 13 14 15 16

- 54 -
Fig. 3. (Continuation)
V. NEWBORN BABY
18.
19.
What do you usually use to cut t~e from his mother? (Check on~y one)
~ 1 BAMBOO SLIVER 2 BLADE 3 FINGERS 4 HOUSEHOLD SCISSORS 5 KITCHEN KNIFE
How is the instrument for cutting using it? (Check only one)
~ 1 PASSED THRU FLAME 2 SOAKED IN DISINFECTANT 3 BOILED 4 SCALDED 5 ALCOHOLIZED
baby's cord to separate him
~ 6 :~~7::::1 KNIFE 7 ,,i-1.L·J,'-'.
8 SCA.EPEL; 9 SURGICAL SCISSORS 10 --------
the cord usually prepared before
~ 6 SOAPED AND RINSED 7 WIPED TvITH WET CLOTH 8 WIPED WITH DRY CLOTH 9 NONE 10 --------~
20. What was the length of the baby's cord left to dry and to fall off? (Check only one)
§ 1 V§ INCHES 2 2 INCHES 3 3.5 INCHES § 4 LESS THAN 1 INCH
5 UP TO BABY'S FOREHEAD 6 INCHES
21. Do you usually apply something to the cord that may hasten its drying and falling off?
21.1
n 1 YES, FREQUENTLY o 3 No, NEVER D 2 YES, SOMETIMES
If YES, what is usually applied on
~ 1 ALCOHOL 2 ANTISEPTIC 3 ANIMAL/FOWL DUNG 4 ASHES 5 CHEWED BETEL NUTS
the cord? (Check only
~ 6 HERBS IN OIL 7 LEUCOPODIUM 8 TALCUM POWDER 9 PURE OIL 10
one)
--------22. Do you usually give medicines/herbs to the newborn to drink?
D 1 YES, FREQUENTLY D 3 NO, NEVER [J 2 YES, SOMETIMES
22.1 If YES, what are these medicines/herbs given and for what purpose?
Medicine/Herbs
23. If suddenly the newborn baby gets cause of the illness? (Check only
§ 1 EXPECTED OF NEWBOR:.1 Lii'E 2 EVIL SPIRITS 3 VISITOR'S PRAISE OF BhBY
Purpose
sick, what could be the possible one)
§ 4 BAD AIR, WEATHER S INFECTION 6 --------
18.
19.
20.
21.
21.1
22.
22.1
23.

- 55 -
Fig. 3 (Continuation)
24. For how long do you usually take care of the newborn after their delivery? (Check only one) § 1 1-.< DAYS §~ 3 WEEKS
2 4-7 DAYS 4 WEEKS 3 2 WEEKS
25. When do you think a mother should start giving soft foods to her baby? (Check only one) § 1 LESS THAN ONE MONTH § 4 ?-9 MONTHS OLE
2 1-3 MONTHS OLD 5 10-12 MONTHS OLD 3 4-6 MONTHS OLD 6 AFTER ONE YEAR
26. What foods do you think are good for the baby?
27. What foods do you think are not good for the baby and therefore not given?
24.
25.
26.
27.
28. Were all of the births you have assisted reported to the authorities? 28. (Check only one)
D 1 YES., ALL D 3 NO., NONE D 2 YES., NOT ALL
28.1 If YES., who usually reports the
[l 1 HILOT ON REQUEST 0 2 HILOT EVEN IF NOT REQUESTED
28.2 If NO., Why not? (Check only one)
0 1 RESIDENCE TOO FAR D? I DON'T KNOW HOW
birth? (Check only one)
0 3 RELATIVE OF PARENTS 0 4 PARENTS
0 3 NOT IMPORTANT D 4 PARENTS' RESPONSIBILITY
29. Do you usually keep a written record of the deliveries you have assisted?
0 1 YES., ALWAYS D 2 YES., SOMETIMES
D 3 NO., NONE
28.1
28.2
29.
29.1 If YES., where do you usually record your assisted deliveries? 29.1 (Check only one)
n 1 CALENDAR n 43 NOTEBOOK 0 2 PAD., PAPER O 29.2 If NO., Why not? (Check only one)
~ 1 NOT IMPORTANT., RELY ON MEMORY 2 NO PAPER., NO PENCIL ! DON'T KNOW HOW TO WRITE AND READ
29.2

- 56 -
Fig. 3 (Continued)
VI. POST DELIVERY OF WOMAN
30. For how long after de!.,-~-"·er-;:, ao ycu usua:::y mke care of the mother 30. (Check only one)
~ 5 :iZ'R WEEKS 'J :r/E WEEKS 7 SIX~ ~TSEKS Q ~T;'C!?'I WE•'EKS _,. ~- • . : .... di LJ
31. Do you usually give medic{n.es, herbs or spec-(al food to the newly 31. delivered woman? (Check :'.)',::2' one)
0 1 YES, ALWAYS 0 2 YES, SOMETI:V:ES
D 3 NO, NEVER
31.1 If YES, what are these and for what purpose? 31.1
MEDICINE/HZ.9.BS/?OOD PURPOSE
31. 2 If NO, why not? (Check only one) 31. 2
n 1 NOT NEEDED B 43 NOTHING To OFFER
D 2 I DON'T Z'l:JW
· 32. What changes in the newly delivered woman indicate that there is 32. something wrong in her return to "normal"?
33. What steps do you usually take ~n this situation? (Check only one) 33.
TREAT IT LEA VE IT ALONE, THE CONDITION USUALLY DISAPPEARS PERFORM RITUALS REFER TO HEALTH PERSONNEL OR HEALTH FACILITY
34. Do you perform some measures to hasten the restoration of the woman to "normal"? (Check only one)
n 1 YES, ALHAYS 0 2 YES, SOUETIMES
D 3 NO, NEVER
34.1 If YES, what are thes;;; .n:ea:s:.:res or procedures and for what purpose? 34.1
PURPOSE

- 57 -
Fig. 3 (Continuation)
34.2 If NO, why not? (Check only one)
§ 1 NOT NECESSARY . 2 I DON'T BELIEVE T.HEY ARE OF BENEFIT 3 I DON'T KNOW HOW, AND WHAT 4 DANGEROUS TO WOMAN 5 ~~~~~~~~---,-~~~
VII. FAMILY PLANNING
35. Have you heard about family
n 1 'lES D 2 NO
planning? (Check only one)
rl 3 I DON'T KNOW D 4 AM NOT SURE
34.2
35.
35.1 If YEE, what does family planning mean to you? (Check only one) 35.1
36.
3 AVOIDING SEXUAL CONTACT § 1 LIMITING, SPACING PREGNANC'l 2 DISOBEDIENCE OF GOD'S LAW
4 INTRUSION IN PRIVATE LIFE JF ';JUPLES 5 ~~~~~~~~~~~~~~~~~
Many couples do something children. Do you approve
n 1 APPROVE D 2 DISAPPROVE
to space pre'JY',ancy or limit the number of 36. or disapprove their action? (Check only one)
rl 3 NO COMMEN1' 0 4 I DON'T KNOW
37. Have you ever advised women to space or limit pregnancies? 37.
0 1 YES O 3 MAYBE [J 2 NO D 4 T DON'T REMEMBER
37.1 If YES, under what circu~stances did you advise them? 37.1
~ 1 DIFFICULT PREGNANCY ~ 5 MARITAL CONFLICT .. 2 DIFFICULT LABOR 6 CONSERVE MOTHER'S HEALTH 3 POVERTY . 7 FOR CHILDREN'S SAKE 4 ILL HEALTH OF PATIENT 8
~~~~~~~~~~~~
37.2 If NO, why have you not ever advised women to space or limit, 37.2 pregnancies?
1 NOT MY RESPONSIBILITY. IT IS THE COUPLE'S AFFAIR 2 DON'T KlWfi HOFl AND fiHAT METHODS TO ADVISE 3 AGAI!lST ldY COllSCIEl{CE~ RELIGION 4 MARRL4GE ME/,NT IC 3EGET CHILDREN 5 l.JIGliT LOSE OI? !JECRE!-..SE J.Jy IlVCOME
38. Do you know of any T'Iethoi ::-::;:::: co~-:-:>les might use to avoid or postpone pregnancies?
D 1 YES
1 ABSTINESC~ 2 PROLOl'lGE!J Ll~_CT_4.TI0~'"'7
5 IUD e HE.PBS
D 2 P70
? ':;Q,_,·.-DCl-l 8 j]TJ,~,=-:'PLG,' .. 1/~!.PS
L, q~~~·.r1CT:JALS 10 ?ILL -, !:BORTION 12
38.
38.1

- 58 -
Fig. 3. (Continuation)
38.2 If YES or NO, would ycu ce interested ~o learn about methods 38.2 of spacing or li~i~ing pre;r~~ncies?
n 1 YES O 3 MAYBE [J 2 NO [J 4 AM NOT SURE
VIII. OTHERS
39. For the past year, have you suggested to your people to go to a 39. health center, clinic, or hospital for maternity care or for any health problems? (Check only one)
0 1 YES [J 3 I DON'T REMEMBER [J 2 NO
39.1 If YES, why did you suggest their going to a health facility 39.1
~ 1 FOR PRENATAL CARE 2 CASE HAD COMPLICATIONS 3 CASE DID NOT RESPOND TO MY TREATMENT 4 DON'T KNOW HOW TO HANDLE CASE 5 .
39.2 If NO, why not? (Check only one) 39.2
~ 1 CEN.TER, CLINIC, TOO REMOTE FROM COMMUNITY 2 KNOW HOW TO HANDLE CASE 3 HEALTH PERSONNEL NOT ALWAYS AVAILABLE 4 ~~~~~~~~~~~~~~~~-
40. Would you be willing to work with the staff of the health center 40. in a program that would help mothers to have easier, safer deliveries and have healthier babies? (Check only one)
0 1 YES O 3 MAYBE [J 2 NO [J 4 I DON'T KNOW
Source: See note 11.

- 59 -
Fig. 4. Translation of questionnaire used for a survey of the knowledge and practice of TBAs in a rural area of Mexico
SURVEY OF EMPIRICAL MIJWIVES
1. Midwife's name
2. Address: Municipio Locality
Street name or any other indication that will ce of help in finding
3. Age last birthday
4. Schooling (number of years)
5. Can you read?
6. Marital status
7. How many live children do you have?
8. How many births have you attended this year (since January 1974)
And in the last month?
9. When was the last time you attended a birth?
10. Name all the localities where you attend births
11 . Have you had any training in a clinic or hospital?
Where? When?
Duration?
12. What type of training was it?
Did you receive a diploma or certificate?
13. Have you attended a special course for empirical midwives?
Where?
Certificate?
14. Since when have you assisted at chi2jbirths?
Do you keep a list of the birt\s attenoed? In other words, do
you write them jown?
15. How do you know a woman is ~~c~~~r~?
16. Do you usually see the ;notl-Jer __:...L .:_ .. E ths :.Jrsgnancy?
Starting in which month?
17. In these cases, what type of help~- ycL g~vs to the pregnant woman?
18. Tell me all the things you do. ~hat j:.J y:u de first?
And after?
Anything else?

Fig. 4. (Continuation)
PRENATAL CARE
- 60 -
19. How do you know if the-pregnancy is going well or not?
20. What do you do when the pregnancy is not going well?
21. If the mother bleeds during the pregnancy, what do you do?
22. If the mother has oedema, or has a bad headache, what do you do?
23. If you ever send a pregnant woman to the doctor or the hospital;
tell me where
24. Do you usually feel for the child?
during the pregnancy?
How many times
25. What advice do you give to a pregnant woman? ~~~~~~~~~~~
26. Do you receive something in retur~ for this help before childbirth?
CHILDBIRTH
27. Tell me all the things you do when you go to a home to attend a
normal birth
And what else?
Anything else?
28. How do you know if the woman is in labour?
29. From what moment do you stay with the mother?
30. Show me all the instruments you use for attending childbirth
31. How do you prepare the mother for the birth?
32. How do you arrange the place where you are going to attend the
birth?

- 61 -
Fig. 4. (Con~inuation)
33. What do you give the mother to ensure an easy birth?
34. How do you know if the birth is not proceeding normally?
35. What do you do in this case?
36. What do you regard as a difficult or complicated birth?
37. What do you do in this case? Explain step by step
38. Have you ever seen cases of haemorrhage?
39. Have you ever seen prolonged labour?
What do you -do in these cases?
40. When and how do you cut the umbilical cord?
41. What do you put on the umbilical cord so that it dries and falls
off more quickly?
42. Do you usually put drops in the child's eyes?~~~~~~~~~~-
What drops? ~~~~~~~~ For what purpose?
43. What do you do to make the child cry when it is born?
44. How do you know if the child is in good health or is sick?
45. What do you do when the child is sick?
46. When do you place the child at the mother's breast?
47. Why do some children die shortly after birth?
48. For how long do you let the mother push without any progress
before you seek help?
PRACTICAL QUESTIONS
49. What do women give you for your assistance during childbirth?
50. How long do you wait for the placenta to come?

- 62 -
Fig. 4. (Continuation)
51. If the placenta dcas ,ot come, what de vcu do?
52. How do you know if the ~lacenta is complete?
53. How do you know if there is haemorrhage during or after the birth?
54. What do you do when the woman bleeds abundantly?
PUERPERIUM
55. After the birth, do you visit the mother?
How often? For what purpose?
What else do you do?
And what else?
56. ·Do you do something to help the mother produce enough milk to
suckle the child? What? ~~~
57. For how many days do you advise her to stay in bed?
58. What food do you recommend to the mother after the birth?
59. What do you do in a case of puerperal fever?
If there are other problems?
GENERAL
60, Do you know that there are health centres provided by the
Government's Social Security Assistance?
Where are they?
What services do they offer?
61. Have you or one of your family ever been to one of these centres?
62. Have you ever sent a patient there?

- 63 -
Fig. 4. (Continuation)
63. What is your opinion of these centres?
What else?
64. Where do you send difficult cases?
65. Do you know it is possible to avoid pregnancy for as long as you wish?
66. What methods (or things) have you heard of for avoiding pregnancy?
67. Have you heard of the pills used for family limitation, intra
uterine devices, condoms, injections, rhythm?
(Indicate the ones you know)
68, Do the mothers ask you for methcds of avoiding an increase of
family?
69. Which method do you recom"end as most effective?
70. Where do you send the mothers for these services?
71. Hav~ you ever used one of these methods? Which?
72. What do you think about these methods for avoiding pregnancy?
73. Do you think people would be more interested in using these
methods if they didn't have to go so far for the service?
Source: See note 12.

- 64 -
Fig. 5. Translation of questionnaire used for an enquiry among women, many of whom were clients of TBAs, in a rural area of Mexico
STUDY OF 300 WOMEN OF REPRODUCTIVE AGE CURRENTLY LIVING WITH HUSBAND OR PARTNER
1. What is your age (age -last birthday)?~~~~~~~--------------
2. Do you have a husband?---------------------------~
3. Do you have Social Security? ___ _ ISSSTE? ---- FF. CC? --------Other type of insurance?-------------~----------~-~
4. How many children have you had? ____ _ How many of them are still alive?
5. Did you attend school? __ _ (yes) (no)
(If the answer is yes, ask) How many years of school did you complete? __ _
6. Can you read? _____ _ (yes) (no)
7. In case of pregnancy and childbirth, from whom or from where can one receive help? (Name all the places and persons able to provide help)
a) (If she does not mention a health instittti.on, ask) Do you know there are
government (SSA) health centres?---------------------~-
b) (If she does not name empirical midwives, ask) Do you know there are
empirical midwives? _____________________________ _
c) (If she does not mention private physicians and nurses qualified to attend
childbirth, ask) Do you know there are pr_ivate physicians and nurses
qualified to assist in childbirth? _____________________ _
d) Comparing the services of the SSA, of empiri';al midwives,and of private
physicians, which of them do you think gives the best service, and which
the worst? ___ ~------- Why do you think that is the worst? ____ _
8. From which of these services would you prefer to receive care during child
birth if you had the means (financial and other) to do so?
Why? _____________________ ~_
9. In general, what do you think people feel about SSA services?~-------
10. In general, what do you think the people feel about empirical midwives?

Fig, 5, (Continuation)
YOU SAID YOU HAVE HAD CHILDREN. I WOULD LIKE YOU TO TELL ME ABOUT ALL THE PREGNANCIES YOU HAVE EVER HAD STARTING WITH THE MOST --RECENT. HAVE YOU BEEN PREGNANT SINCE YOU LAST GAVE BIRTH?
1 2 3 4 5 6 7 8 9
Last Pregnant Abortion Born Liveborn Liveborn and During the pregnancy Did somebody attend Did somebody attend you pregnancy now dead but died survived the did you have prenatal you during the child- during the period
within first 10 days supervision? Yes birth? Yes --- following the birth? From --
10 days of No If Yes, No (If yes)Who? Yes No what Now alive -- -- --- ---
birth . --- ( If yes) Who? cause?
dead? Why?
What·was or ..
Where? the cause What was the
' of death? cause of death? Where?
From whom? When and how many times?
Was the birth a normal one or did you have complications1
At what age? What did the person do? Where? Normal
Complications
( If complications) What kind of
What com-
treatment or plications? Did somebody examine the . ' advice were you given. baby? Yes No --- --
( If yes) Who? ( If complications) What was done about When and how many times? them?
Were you satisfied with the service you received? (If attended) Are you Was the baby vaccinated?
satisfied with the Yes No ---care you received? ( If yes) By whom? ___
i How many times?
i, Do you breastfeed the baby. Yes No -(If yes) Until what age?
Source: (See note 13.)

- 66 -
Fig. 6. Some existing practices among TBAs and proposals for their modification, as seen by a group of public health nurses
Existing practices
1. Advice prior to marriage a) Provides, but advice is in
accurate or inappropriate
b) Does not provide
2. Prenatal care a) Advises on nutrition but lacks
knowledge and encourages adherence to taboos, some of which are unsafe, e.g., discourages protein consumption
b) Gives incorrect advice on personal hygiene, e.g., advises against bathing, encourages the use of too hot water, etc.
c) Administers local potions without awareness that some may adversely affect development of the fetus
d) Does not recognize danger signs and symptoms
3. Delivery: first stage a) Does not arrange instruments for
the delivery and does not ensure cleanliness of instruments and site of delivery
Proposed modifications or additions
Advice should be continued but made more accurate and appropriate and include advice on the timing and spacing of pregnancies and on preparation for parenthood
Should learn to give advice as indicated above
Should learn essential principles of nutrition and advise mothers accordingly, encouraging the continuation of safe taboos and discouraging that of unsafe ones
Should learn about essential elements of personal hygiene and advise mother accordingly
Should learn about and suggest the use of available harmless drinks
Should learn to recognize danger signs and symptoms and make an early referral to nearest health service
Should learn about the need for cleanliness of instruments and of place for delivery and do what is necessary to ensure same
b) Tries to hasten labour by various Should learn about the approximate means, e.g.: duration of normal labour and should
not try to hasten it. Mothers experiencing prolonged labour should be referred to health services
- administers herbal concoctions, some of which may hasten labour when not warranted or may otherwise be harmful
- squeezes uterus forcefully, or places tight bands on epigastric region, or pulls on limbs
- encourages or administers hot baths inserts tampons of local concoctions into vagina
- should administer harmless drinks
- should substitute gentle massage and include areas other than the uterus
- should encourage or administer tepid baths only
should insert nothing into vagina

- 67 -
Fig. 6. (continuation)
Existing practices
- administers marketed drugs without knowing their intended use and effect urges mother to bear down before the time to do so is right
c) Does not recognize early danger signals
d) Does not ensure the presence of additional help in the home if needed
4. Delivery: second stage
5.
a) Tries to hasten birth by: - external pushing on uterus - manual dilation of cervix - use of foreign matter to
lubricate birth canal - deliberate rupturing of
amniotic sac (by fingernails, pins, etc.)
b) Forces the mother into uncomfortable and otherwise unsuitable positions for delivery
Delivery: third stage a) Cuts the umbilical cord in in
appropriate ways, e.g.: with an unclean instrument, or in the wrong place, or at the wrong time
b) Tries to force extraction of placenta by, e.g., massage, manual extraction, introduction of lubricants, other local
i.1ethods
Proposed modifications/additions
- should not use marketed drugs
should learn about the signs that indicate the time for bearing down and should encourage and help the mother to walk about gently until the time for bearing down is right
Should learn about early symptoms pointing to complications and refer mother to health services when such symptoms are manifest
Should learn about the importance of having a helping hand and should encourage the husband (or other adult relative or neighbour) to be present and assist where necessary
Should learn about approximate normal interval for second stage of deljvery and, if this is prolonged, should refer the mother to health services. Should learn abou dangers of manual interference, refrain from such interference, and encourage mother to breathe deeply
Should learn about and ensure that the mother is in a position that is comfortable and culturally acceptable and that will facilitate delivery
Should learn the essentials concerning cleanliness in dealing with the cord, the way to ascertain the best time to cut it, and the place to cut it, and should apply what she learns
Should learn not to hasten delivery of the placenta by manual or other manipulations but to observe carefully and ensure that the e,,tire placenta is delivered

- 68 -
Fig, 6, (continuation)
Existing practices
6. Care of infant at birth a) Ties and dresses the umbilical
cord with unclean materials (e.g., cowdung, saliva, ashes for dressing) or heavily cauterizes it
b) Uses inappropriate methods to make child cry (breathe), e.g., dips in cold water
c) Uses inappropriate methods and materials for cleaning the eyes
d) Administers purgatives to the newborn
e) Leaves child without food or water for several days
f) Leaves child unclothed
g) Fails to look for or detect deviations from the normal
7. Postnatal care: mother and child a) Considers puerperal fever as
"normal"; does not recognize damage to genital tract
b) Encourages extremes in maternal hygiene, e.g., bathing in very hot water, or not bathing for .40 days
c) Externally manipulates tru:,k and pelvis
d) Encourages either too early ambulation of mother or prolonged bed rest (about ~O days)
e) Encourages nutriticnal taboos, some of which may be harmful
Proposed modifications/additions
Should learn to tie and dress cord correctly and with clean materials, to cover with a clean cloth, and to refrain from cauterization
Should learn and apply simple methods of resuscitation
Should wipe eyes gently with clean cloth dipped in cold boiled water
Should give plain boiled water with sugar
Should encourage breast-feeding and give additional liquids
Should keep child warm
Should learn about the normal baby and develop skills in observing and detecting abnormalities
Shculd learn to recognize danger signs and symptoms and refer the mother to health services
Should encourage moderation in bathing and the use of tepid clean water
Should learn and apply appropriate methods of massage in moderation
Should encourage gradual ambulation and moderate activity, with rest in between
See 2a.
f) Fails to encourage breast-feeding Should encourage breast-feeding
g) Provides advice on pregnancy spacing that is harmful and/or ineffective
Source: See note 22.
Shculd learn and advise accordingly about appropriate sexual behaviour and modern family planning methods
Remark: The above is a modified version of what appears in the source cited. Unlike the original, it reflects only unsafe or otherwise inappropriate practices, i.e., those that need modification. Neither any one nor all of the above practices apply to all TBAs. 1'he good practices of
many TBAs include, in addition to some of those listed in the second column, housekeeping tasks and emotional support of the mother and her family.

- 69 -
Fig, 7, Example of a learning module
Example 1: "The badly fed child 11 {see Part I, Problem. 3,2)
Learning objec,tives
To be able to: -weigl} a
child -decide whe
ther the child has the right weight for hi.sage
-recognize 3 major signs of malnutrition
-show a mother how to prepare a bottle of liquid to feed a child suffering from malnutrition
-tell in what cases a PHW would send a child suffering from severe malnutrition to the hospital or health centre.
Finding out content U8ing what a what the FHW f--'-( a_s~f!'_om_t_h_e_hl_or_k~i_nge....Gl.l_id_e J ___ ~ PHii ha8 already knows aLready
Learning/teaching m«thods*
about this Whot a FHW must What a PHW must Lea:I'f'llld problem know do
Has he seen a malnourished child? or heard of one? What did he look like? What was done for the child? Did he get better or worse or died?, etc.
;
Review briefly the growth and development of a child, Early signs of malnutrition: -persistent
crying -diarrhoea -getting
thinner -not growing
well Sever signs of malnutrition: -skin creases
(the child just skin and bone)
-eyes dull -does not
eat -vomits -diarrhoea -fever -swelling of
Exa.n1ine a child Weigh a child Use weight chart Talk with mothor Demonstrate how to prepare food for child and how to give it and return demonstration by the mother
lGi ve liquid ]mixture (water, ioil, condensed milk) Give medicine Prepare and clean equipment Send sick child to hospital or health centre
legs, feet and hands
-hair changes colour
Treatment: -replacing lost
liquid 1;
-changing or ! correcting j child's · diet
Signs of improve mentor getting I worse When and where to
refer? I How to organize a community gathering for health teaching.
Source: See note 26.
-How to com- Lobservation of how pare the r mothers feed their weight of children (house, dis-
I
healthy per.sary, market) and child with talk to them the age of the child -How a baby grows and develops -The wellfed child -Local food customs and habits -AdvantagM of birth spacing for mother and child -Nutrition
eFind out local food habits and customs, whit: food available (special a11signment) watching ard giving demonstration
eTalking with people about healthy nutrition
eGetting the help of the agricultural extension worker to teach local people- to grow food
ePractise work in a dispensary, home visiting,
leGroup discussion (students talk about the growth and development o,f children, their own or others)
ePlily acting
Give to each method listed here a priority number in order to begin by the ones you consider the most important and leave aside those you may not have enough time to deal with.
Har.> is the PHW progreesing (Evaluation}
Ways of evaluating this:·
Observation of the PHW -During weighing the
child: Did he check that the
scale is balanced Did he hold the child safely
Did he talk with child and/or his mother
~id he read the correct weight and write it on the chart?
-How did he examine the child, e.g. did he press the skin to see if swelling of the leg is there, or if the skin creases?
-How did he teach the mother about giving fluid to her child, did he show her how to to do it?
-Did he prepare and clean equipment?
-Practising other tasks: Giving fluid or medicine, demonstrating about food with the mother at home and/or women in the comm.unity.
questioning oral and Written, and listening
-Is the we;ght of the child correct for its age? if not, why not?
-What would you do for him?
-How would you know if he is improving?
-How can you tell it is becoming serious? what would you do for him?
-What can you do to prevent this problem?
-What can the mother do? -What can the community
, do? and who can help? l -Wh5t did you know about l this problem in your l special assignment?

- 70 -
Fig. 8. Sample checklist to assess _a TBA' s performance during a delivery demonstration in the home
Name of TBA Observed by -------------
Location of TBA Date of observation----------
A. Recognition of onset of Labour 1. Inquires about the presence and duration of
- backache or abdominal cramps - pink discharge or "show" - uterine contractions - breaking of "bag of waters"
2. Examines the abdomen to determine - position of baby - duration of contractions - severity of contractions
B. Preparation for delivery 1. Selects site for the delivery that is
- quiet, clean, ventilated - uncluttered,with adequate space for
arranging supplies
2. Prepares equipment for the delivery - scrubs hands - removes contents of delivery kit - boils scissors 10 minutes - arranges items for easy reachability - covers supplies with clean cover until
ready for use during delivery - obtains container for waste - covers delivery site with clean material
3. Prepares herself for delivery - covers hair - scrubs hands thoroughly prior to
preparation of mother - performs additional hand-scrubbing as
necessary during delivery - puts on clean apron or the like when
delivery is near
4. Prepares mother for delivery checks if mother bathed early in labour
- helps mother to bathe if needed - cleanses vulva with safe cleansing
agent and water - uses downward strokes in cleansing - discards each swab after use - gives fluids throughout labour
Performance Comment
Plus* Minus* N.O.*
*"Plus" can mean either "yes" or "satisfactory". "Minus" can mean either "no" or "unsatisfactory". "N.O." means "not observed".

- 71 -
Fig. 8. (continuation)
C. Care to mother in Labour Provides appropriate care during labour - provides backrub for comfort - helps mother to change position as
necessary - provides emotional support to mother - relates to family members in culturally
prescribed manner - avoids unnecessary interference with birth
process such as - strong massage of abdomen - insertion of hands into birth canal - administration of medications
D. Recognition of normal progress during birth 1. Palpates abdomen to determine
- baby's position - quality and duration of
contractions
2. Observes perineum for abnormal bleeding
3. Recognizes danger signs during labour - prolonged labour - convulsions during labour - breech or shoulder presentation of baby - prolapsed cord
4.Responds appropriately to complications of delivery - summons midwife or physician if possible - initiates appropriate care until help
arrives
E. Performance of safe, hygienic delivery 1. Prepares for delivery
- puts on clean apron - thoroughly scrubs hands - watches perineum for appearance of
baby's head
2. Prevents perineal laceration - applies gentle pressure to baby's head
to slow the delivery - instructs mother to pant so as to
reduce speed of delivery of head - applies gentle manual support to
perineal area
Performance Comment I Plus* Minus* NO*

- 72 -
Fig, 8. (continuation)
3. Delivers the baby - supports the head as it emerges - feels around baby's neck for cord - gently slips cord over head if it was
found around neck - removes sac from head if it is present - wipes baby's eyes, nose,and mouth with
clean swab as soon as head emerges - supports baby as its body emerges - inverts baby to drain mucus - places baby on clean cover between
mother's legs
4. Attends to umbilical cord - washes hands before manipulating cord - tests cord for cessation of pulsations - avoids contamination of cord ties - applies cl~an cord ties - ties square knots in applying cord ties - checks knots for security - lifts scissors by handles, avoiding
contact with blades - cuts cord between the two cord ties - observes cord stump for bleeding - touches only edges of cord dressing - applies dressing,with cord in "turned
up" position - avoids unsafe pr.ac tices in cord care
such as application of unclean materials, earth, saliva, ashes
5. Prevents haemorrhage - puts baby to mother's breast to
stimulate uterine contraction - identifies separation of placenta by
watching for small gush of blood from birth canal
- avoids pulling on placenta or membranes as placenta emerges
- catches placenta in basin - inspects placenta carefully to see if it
is complete - examines placenta for evidence of foul
odour - inspects external genitals for fresh
bleeding or lacerations - palpates uterine fundus frequently for
hardness - massages uterus gently to _control
excessive blood loss - avoids unsafe practices such as packing
birth canal to stop bleeding
Performance Comment
Plus* Minus* N.O.•

- 73 -
Fig. 8 (continuation)
. I f Per ormanci Comment.
I F. After-care of mother Promotes mother's comfort after delivery - wipes perineum with clean swabs
uses downward strokes in wiping perineum - sponges mother
changes mother's clothing - provides clean mat to lie on - applies clean pad to perineu..~ - offers food and drink - provides opportunity for rest
Plus*
-·--"'---_ _,,__ __
Minus* N.O. *
! :,----..--.,..., . .., . ----r-·-··~ ~-
__ J

- 74 -
Fig. 9. Sample checklist to assess the use and care of the delivery kit
or bag by trained TBAs.
Village of TBA---------~~~~-
Place a (v') in appropriate column
1. Utilizes own delivery kit? 2. Washed hands before touching contents? 3. Kit is clean? 4. Contents of kit are clean? 5. TBA record book is carried outside kit
Items in kit
1. Basin/large bowl 2. Cleansing agent or soap 3. Towel 4. Head cover or any appropriate material 5. Apron 6. Eye medication 7. Supply packet containing
- cotton balls - gauze swabs
sharp blunt-point scissors or blade - container for boiling
8. Cord dressing packet containing - cord ties - cord dressings - cotton balls
9. Tray cover
Date of observation ------
Observed by-----------
"es No.
-
Correctly Item described
c...·P>resent use of item
Yes No Yes No
* This is only a sample and far from complete. Items may be added or deleted, according to the situation.
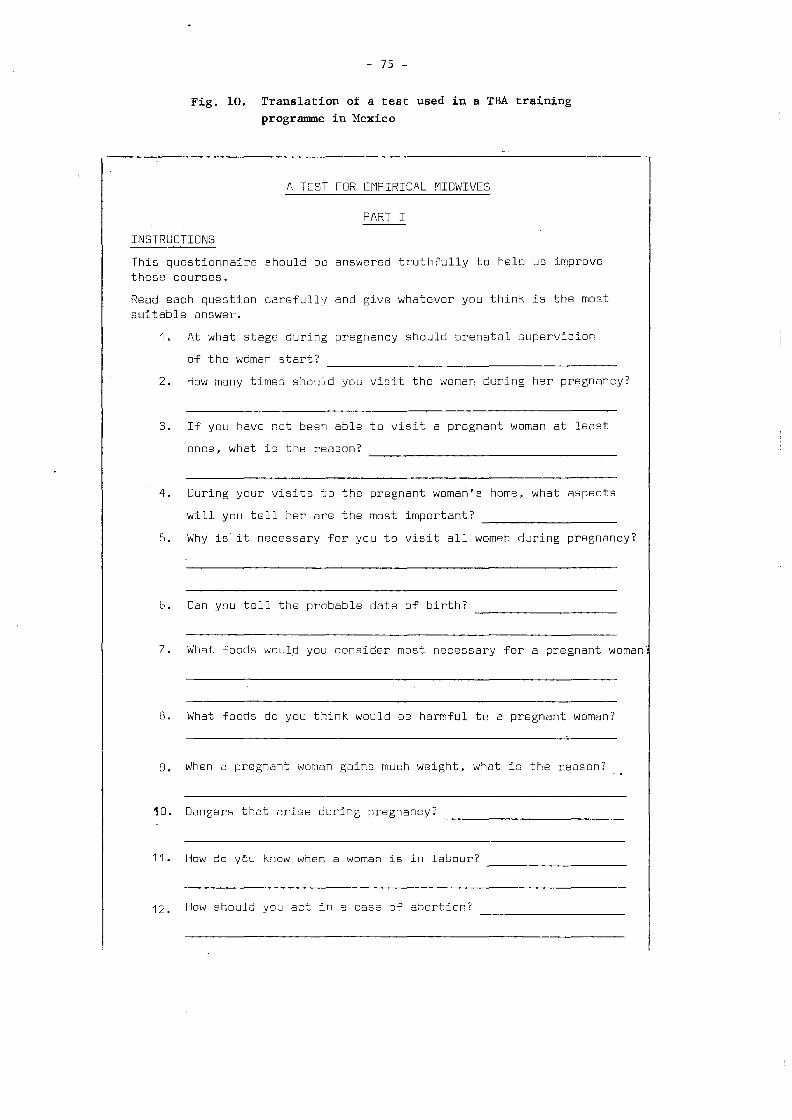
- 75 -
Fig. 10. Translation of a test used in a TBA training programme in Mexico
A TEST FOR EMPIRICAL MIDWIVES
PART I
INSTRUCTIONS
This questionnaire should be answered truthfully to help us improve these courses.
Read each question carefully and give whatever you think is the most suitable answer.
1. At what stage during pregnancy should prenatal supervision
of the woman start?
2. How many times should you visit the woman during her pregnancy?
3. If you have not been able to visit a pregnant woman at least
once, what is the reason?
4. During your visits to the pregnant woman's home, what aspects
will you tell her are the most important?
5. Why is it necessary for you to visit all women during pregnancy?
6. Can you tell the probable date of birth?
7. What foods would you consider most necessary for a pregnant woman
8. What foods do you think would be harmful to a pregnant woman?
9. When a pregnant woman gains much weight, what is the reason?
10. Dangers that arise during pregnancy?
11. How do you know when a woman is in labour?
12. How should you ac~ in a casa 8f abortion?

- 76 -
Fig. 10. (Continuation)
13. How do you prepare the patient before the birth?
14. Do you make a vaginal examination?
15. What do you need for attendance at childbirth?
16. What is your attitude during the labour process?
17. What do you do when, during the birth, the cord appears first?
18. What do you do when, during the birth, there is bleeding?
19. What do you do when, during the birth, there is an abnormal
presentation? (face, arm, or breech]
20. When the placenta stays inside for an hour, what do you do?
21. How do you know if the placenta is complete?
22. What do you do when th~ woman bleeds very much after the birth?
23. What do you do when the woman has fever after the birth?
24. Why must the scissors for cutting the cord be sterilized?
25. What medicine do you apply to the umbilical cord of the child?
26. What treatment do you give to the eyes of th~ child?
27. Why do you put drops in the child's eyes?
28. What do you use for extracting the child's phlegm?
29. What do you do when the newborn child does not cry?

- 77 -
Fig. 10. (Continuation)
30. What food do you consider best during the first six weeks after
birth?~---'--~-------------------------~
31. What do you do when the .child has colic?
32. What should the baby's diet be in the third month?
33. After how many months should ths mother supplement her breast milk
with other food for the baby?
34. What ~enefit does the child receive when he is breast-fed?
35. At what age do you think the child should start to receive
medical check-ups?~---------------,----------~
36. What advice do you give the mother when the child has diarrhoea? ---
37. What methods do you know for avoiding pregnancy?
38. WhEcJre do yri11 send persons who would like information about family
. planning?
39. Do you think it would be good to keep in touch with the medical
service of the IMSS (Mexican Institute of Social Security)?
40. What is the object of participating in a community group?
41. Why is it important for you to maintain contact with the health
institutes?
42. For your work as a rnidwife, with what pecple should you be in
touch meinly?

- 78 -
Fig. 10. (Continuation)
43. Why did you come to this course?
44. How did you find the subjects you were taught?
45. What is your opinion about the instruction you received?
46. During the lectures, did you ask about what you did not understand?
47. Did you understand the lessons given by the instructor? ~~~~~
48. What is your opinion about the practices and demonstrations?
49. Do you think the place where you took the course was adequate?
50. Why?~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did you obtain what you expected from this course?
51. Have you noticed any change in yourself after the training?~~~
52. What activity of the course did you like best?
53. What bothered you most in the course?
54. How do you suggest these courses be improved?
Source: See note 28.

- 79 -
Fig. 11. Page from an illustrated manual for TBAs in the Philippines
T\'INt; l•'IUST LOOI' OF SQUARE KNOT
STEP 1
STEP2 S7EP3 STEP4-
5TEPS sr~P6
17
DOH/IH & MS - Divi,ion of Maternal and Child Health, .... Ila.
Source: See note 29.

- 80 -
Fig, 12, Illustration from a WHO manual for the training of primary health care workers
Source: See note 26.
One breast hurts a lot
Tell the mother to squeeze the milk from the breast with her hand and to then give this milk to her baby
She should put hot compresses on the breast that hurts: 3 or 4 thicknesses of cloth dipped int; hot water (but not burning hot!) She should do this for 10 minutes and do it about 3 or 4 times a day

- 82 -
Fig. 14. Translation of form used in Costa Rica for making an annual report on a TBA
MINISTRY OF HEALTH
DEPARTMENT OF MATERNAL AND CHILD HEALTH
SAN JOSE, COSTA RICA
EMPIRICAL MIDWIFE'S ANNUAL REPORT
Name Address
Canton District
Year 19 No. of Carnet
No. of births attended 1,n the presence of a doctor or nursemidwife
No. of births at whr~ch you had to caU the doctor or midwife
No. of births that you attended alone, prenatal care having been given at the heaith centre
No. of premature babies --------------------
(Babies weighing less t~an St lbs)
Source: See note 33.

- 83 -
Fig. 15. Translation of form used by the TBA in Costa Rica to notify the health centre of a birth
NOTIFICATION OF BIRTH
Address
Time of birth _____ _ Sex Weight
Condition of mother after the birth ~~~~~~~-
Condition of the child at birth:
Alive:
Premature
Any defects present?
Name of empirical midwife
Source: See note 33.


Fig, 17. Form used in a programme i.n Central .Java to record the dukun's (TBA's) reported efforts to encourage her clients to visit a family planning clinic
APPENDIX IX
CENTRAL JAVA DUKUN STUDY
PERFORMANCE EVALUATION FORM ( REVISED VERSION, AUGUST 1972)
Serial number of form _ _ _ _ _ _ Name of client ___________ _
Number of living sons _______ _ Number of living daughters ___ _ Total number of living children __
Subdistrict Acceptor registration number __
Name --0f dukun
Village
( referrals only )
Method accepted
Date form started _ _ _ _ _ _ _ _ _ _ Action C
Date first monthly reminder due . ______ _
Date first monthly reminder given. ______ _
Date second monthly reminder due _____ Reason
Date ____ _
Date second monthly reminder given _____ Date_ form discontinued
_ _ _ _ _ _ _ _ Action D Date form filed permanently _____________ _
1. Have you advised the mother about family planning ?
(a) No (b) Yes
D _ _ _ _ _ _ _ _ Action A
D
2. Will she come to us for help ?
(a) Don't know D ________ Action A
(b) No D (c) Yes 0
Source: See note 41.
3. If she will come, why does she want family planning help ?
(a) because she wants no O more children
(b) because she wants to D delay the next pregnancy
(c) because she wants more D information about family planning
(d) don't know O
_ _ _ _ _ _ _ _ Action B
4. If she will not come, is she using one of the following methods to stop becoming pregnant ?
(a) massage D (b) herbs O (c) breastfeedings D
________ Action D
(d) abstinence O (e) other O
-Action A Ensure that a further attempt to complete the form will be made in one month's time. Enter dates when reminders are due and given. Repeat procedure once more if necessary. Then take action D, even if no family planning action has been recommended.
Action B Allow 6 months for client to appear. If she appears and accepts a method, enter acceptor registration number from clinic card, date of registration, and method accepted. Then take action D.
Action C
Action D
In the event of divorce, death, move from village, discontinue form enter reason, briefly, with date. Then take action D.
File form very carefully.
0:, Ul

- 86 -
Fig. 18. Some likely indicators of the quantitati,:e pe:-::ormance of trained TBAs
and the impact of their services on r.22.::._c:-: s:at;1s.
Evaluation of quantity of services
(a) Number of pregnant women referred to health facility at least once for antenatal care, bv:
i) trained TBAs ii) other trained individuals*
iii) untrained individuals
(b) Number of high-risk pregna~c ~omen referred to jealth facility for antenatal care, by: (same three categories as a:,ove)
(c) Number of mothers referred to health facilit·.· sc least once for postpartum care, by: (same three categories as a:iove)
(d) Number of births attented c0:,':
(same three categories as above)
(e) Number of difficult births :-eferred to hea::h facility by: (same three categories as a:::i-ove\
(f) Number of infants referred at least once to health facility by: (same three categories as a·::JVe;
Evaluation of impact
(a) Number of perinatal deaths, per given number of births, where birth attendant ,as:
i) solely a trained TBA ii) solely another trained individual
iii) solely an untrained inciyidual iv) a health service staff ::iem:>er acting on a
referral made by a trained ISA v) a health service staff ~ember acting on a
referral made by an untrained attendant
(b) Number of infant deaths caused b:: tetanus ne·or.a:::,rum, per given number of ir.fa::1t ciea:hs, ,;here ::iirt"::: attendant was: (same five categories as abo,:e:
(c) Number of post-neonatal deaths (29 days or ::icre, but under 1 year), per given nur.i:Jer of live ':,ir:":::s, where birth attendant was: '.same five categories as above)
(d) Number of neonatal deaths '.23 days or less', ?er given number of live births, ~·~:i.ere :iirth at:::er,dar:: was: (same five categories as abovel
Year 1 (prior to start of TBA training
'{ear 2
(posttraining period)

- 87 -
Fig. 18. (continuation)
Year 1 Year 2
(prior to (post-
start of training
TBA training)
period
(e) Number of early neonatal deaths ( 7 days or less but excluding late fetal deaths) per given number of live births, where birth attendant was: ( same five categories as above)
(f) Number of perinatal deaths ( late fetal deaths plus deaths in first 7 days) per given number of live births and late fetal deaths, where birth attendant was: ( same five categories as above)
* The term "other trained individuals" includes individuals (other than trained TBAs) who have had formal preparation, such as professional and auxiliary nursing and midwifery personnel, and obstetricians.

- 89 -
NOTES AND REFERENCES

- 90 -
::;-oms AND REFER&~CES
1. Verderese, Maria de Lourdes &;; Turnbull, Lily ~!. The traditional birth attendant in maternal and child health and family planning: a guide to her training and utilization. Geneva, World Health Organization (WHO Offset Publication No. 18)
2. Professional health personnel may find it difficult to accept the TBA as a legitimate member of the health team, for one or more of the following reasons:
(a) they have been trained in educational programmes based on the Western model of scientific medicine;
(b) they come from a segment of the population that enjoys a higherthan-average standard of living, in social and economic terms;
(c) they have never lived in a rural area and thus have no first-hand knowledge about the conditions in which the poor in their country live;
(d) they are unaware of the magnitude of and the factors underlying the health problems of the poor, and of the dearth of health services for the poor;
(e) they know little about the customs, beliefs, and practices of various segments of the population as regards birth, the maternity cycle, the care of mothers and infants, and the spacing of children in a family;
(f) they have unrealistic notions about the country's capacity to produce and employ a sufficient number of professional health workers to satisfy the needs of the masses for health care; and
(g) they have had no first-hand experience with TBAs and thus know little about the potential of the TBA for providing much-needed health services in areas where professional health workers either refuse to work or, for other reasons, are in short supply.
3. Some of the factors that professional health personnel should be aware of are the following:
(a) the rate at which the population is growing (compared with rates in more developed countries) and the implications of this for health and development;
(b) ratios of physicians, nurses, and nurse-midwives per unit of population in rural areas compared with urban areas (as a measure of the extent to which rural areas are deprived of professional health manpower);
(c) the per capita income of the poorest 30-40~ of the population (as a measure of the inability of the poor to meet basic needs with respect to nutrition, housing, sanitation, and health care - particularly health care provided by expensive health personnel;
(d) infant mortality rates (compared with the rates in more developed countries);

4.
- 91 -
(e) death rates among women of child-bearing age (compared with the
rates for other segments of the adult population);
(f) prevalence of malnutrition and of infectious and communicable
diseases; and
(g) the proportion of births_ that occur without the .attendance of professionally qualified personnel (as a measure of the extent to which other health workers are needed in the area of maternal and child care).
Influentia~ persons or groups in the community might include: the village headman; a council of elders; a council of family heads; a coordinating council covering several villages; religious leaders; organized women's groups; and other health workers in the village, e.g., traditional medical practitioners, primary-care workers, and health educators.
5. The following are_ among the questions requiring -examination as regards
6.
services in maternal and child health and family planning:
(a) What agencies and associations (national and international) are currently providing such services?
(b) What divisions within the ministr_y of health are involved in such services? Possibilities might be the divisions for maternal and child health, family planning, nutrition, community (or public) health, and health education.
(c) What private practitioners (e.g., gynaecologists, obstetricians, and midwives) are providing such services?
(d) What services do the various agencies, divisions, and private practitioners provide - in urban and rural areas respectively?
(e) What is the structure of government services - national, regional and;-or provincial, district, and village? What are the staffing patterns in these services (categories of health worker, numbers employed, and where they are located, particularly with respect to services in rural areas)?
(f) What new categories of worker (e.g. primary care workers and health educators) are being developed and utilized in services for rural areas, and what relationship is envisaged between the work of TBAs and that of the new categorjes?
(g) Are there plans for the expansion of training programmes for the types of health personnel currently working in the field of maternal and child health and family planning (e.g., practical nurses, medical auxiliaries, community health nurses, and auxiliary nurse-midwives)?
Mangay-Angara, Amansia. A study of traditional birth attendants (hilots) in the Philippines: phase I - manpower and registry. Manil~, R~gional Office for the Western Pacific of the World Health Organization, Ll97_i/. (Unpublished mimeographed document). The report_ on the survey states its purposes as follows:
7.
8.
- 92 -
"To obtain baseline information on practising hilots throughout the country as to their number, geographical distribution and characteristics in terms of age, sex, marital status, level of education, their preparation for hilot practice and their activity status.
"To prepare hilot registries at the central and local levels of the health services from the information obtained."
Most of the data were collected by professional midwives, public health nurses, and sanitary inspectors, under the supervision of health service officials. As a result of the survey, the number of TBAs registered was 31 122 out of an estimated total of 40 000 in the country. It was estimated that there was ohe TBA for every 1000 to 1250 individuals in the country. The investigators were surprised to find that male TBAs constituted 16% of the total. Most of the TBAs (81%) were in the age group 40-69 years. Only 49% were described as being able both to read and to write.
The report of the Philippines (note 6 above) indicates that one reason why some TBAs refused to cooperate in the survey was their apprehensiveness towards health authorities, dating from a time when it had been official policy to discourage the TBA from practising.
Those chosen to plan and direct the survey should be capable of assuming responsibility for, inter alia:
preparing the plan of work for the survey, including activity schedules;
providing guidelines on how survey activities can be incorporated into the routine operations of health personnel at all levels of the organized health services;
initiating and following up the procurement of supplies and equipment;
compiling and organizing the existing basic information needed for the conduct of the survey (e.g., estimates of the number of TBAs as a basis for calculating the number of survey forms to be printed; a list of all zones or other equivalent geographical entities, for mailing purposes; a list of the organized health·prograrnmes and services and their location -these being the mechanism through which the survey might most feasibly be conducted; and information on needs for transport);
constructing, pretesting, and refining the data-gathering forms to be used;
planning and conducting (or overseeing) the briefing of collaborating field staff (e.g., regional health directors and health officers in provinces or cities);
developing information materials on the purpose and procedures of the survey and overseeing the distribution of such materials to field staff involved in the survey;
establishing a monitoring system for field activities;

- 93 -
designing the format of the registration card or sheet, if one of the objectives of the survey is the establishment of a permanent register designed to allow updating;
making arrangements for the processing of data;
data analysis and interpretation, the preparation of reports, and the dissemination of survey data to those who need them for planning training programmes and for evaluating such programmes and the impact of the trained TBAs' services on health.
9. Djuarini, S. et al. Report on the study of dukuns in Central Java. Jakarta, Indonesian Planned Parenthood Association, 1971. This anthropological enquiry comprised approximately 100 interviews, most of them with TBAs and their clients but some with community leaders. The investigators found that the TBA was the usual source of midwifery assistance, and that she usually attended 2 or 3 births a month. As well as providing assistance at birth, she was the acknowledged authority on prenatal and postnatal care. Almost always she was middle-aged or elderly. She usually saw her work as spiritual in character, and her knowledge of ritual was an essential element of her expertise. Her work included help and advice with traditional methods of birth control, especially massage (believed by TBAs to affect the position of the uterus), and the prescription of special herbs.
10. Landa Jocano, F. Cultural changes in relation to a sustained country-wide
11.
family planning programme. In: Proceedings of the International Planned Parenthood Federation South East Asia and Oceania Regional Conference, 21-27 March 1971. Manila, Pustamente Press, 1971. According to this report, the peasants believed, for example, that overheating of the portion of the body immediately above the womb resulted in miscarriage if the woman was pregnant. The underlyi-ng theory was that, to remain in good heal th, it was necessary to preserve a state of harmony and equilibrium between the body and elements of nature. The heating of the womb was believed to be one of the many ways in which this harmony could be disturbed, with unfortunate consequences. Another way was by the introduction of alien objects, including the condom and the IUD, into the body.
Unpublished questionnaire supplied by Mrs Nelida K. Castillo, Department of Health; Manila.
12. Keller, A. & Arias Huerta, J. Traditional midwives and maternal and child health in rural Mexico. (Unpublished document, 1977; published in part in Salud publica de -Mexico, ..!.§_: 883-892 ( 1976).) The survey in Mexico was undertaken to provide the Ministry of Health with answers, in respect of "a typical rural area", to the following eight broad questions:
Who are the tradi tioha1 midwives? What- are their socio-economic characteristics?
What proportion of births do they really attend?

13.
- 94 -
How much do they know about correct birth attention? How much of what they know do they practise?
What do they know about family planning and contraceptives and what are their attitudes in this regard?
What would they have to be taught to make them effective maternal care and family planning agents?
What is needed to obtain their collaboration with these programmes?
In the final analysis, can they be effective agents in such programmes?
Specifically with regard to family planning, what roles can they successfully be assigned?
Since there was no prior inventory of TBAs, interviewers were given the task of finding them. The following findings were among those presented in the above document: 60 TBAs were identififed; of these: 37% were describable as "active"; only 55% had a correct idea of how to diagnose a pregnancy; approximately 50% displayed "adequate notions" of how to detect·birth anomalies; while 86% were aware of the existence of government health centres, almost 50% did not know what kinds of services were offered in them, and only 45% had ever sent a patient to such a centre; 70% expressed approval of the use of modern contraceptives; 63% said they would actively cooperate in a government programme to make contraceptives available, and most of the others mentioned their age (25% were aged over 65) as the reason for being unable to cooperate.
Keller, A. & Arias Huerta, J • .2E_.cit. The questionnaire for mothers was one of the methods used to obtain answers to the eight broad questions listed in note 12. It was administered to a representative sample of 200 mothers in the study area, which in 1973 had a population of 48 000 living in 50 different communities. The following findings were among those reported: in 43% of cases, the last livebirth had been attended by a TBA; 48% claimed not to know that fertility regulation was possible; only 15% said they had actually used a method. Over 100 "losses" of pregnancies or deaths of liveborn children were reported for the 200 mothers. In the majority of cases, the loss or death appeared to be attributable to one of the following causes: asphyxia and incorrect positioning of the fetus at birth, respiratory complications of the newborn, and, among young children, gastroenteritis, respiratory complications, and measles. (The authors of the report remark that all these causes are
- "susceptible to elimination through adequate attention during the relevant periods.") According to the questionnaire responses, the mothers had a relatively low opinion of the competence of TB.As and only 10% said they would use them if circumstances permitted a free choice. The fact that so many did use them, instead of available health service facilities, appeared to be due partly to confidence in the particular TBA used and partly to the problems of using professional services. These problems included the high fees that private physicians were said to demand, the unavailability of physicians when needed, and the inability to have a personal relationship with them.

- 95 -
14. Brown, Pauline P. The role of a bhil traditional birth attendant: an approach to collecting initial information pertaining to the identity and functions of traditional birth attendants within a tribal community in Central India. Hamilton (Ontario), McMaster University, 1978 (unpublished document). This report includes not only a comprehensive review of relevant literature (103 references) but a detailed description of methods, important findings, and recommendations. What may be most important for those interested in questionnaire design is the well-conceived interview schedule used in the survey, which would have been reproduced in the present publication if there had been sufficient time to negotiate clearance in this regard. Among the recommendations of the author are those calling for: the establishment of more rigorous criteria for the selection of interviewers; the extension to one week of the training period for interviewers; and the designation of a trained person, such as a public health nurse or auxiliary nurse-midwife, to spot-check the interviewers during home visits in order to determine what difficulties they are encountering.
15. Mukherjee, B.N. Reliability estimates of some survey data on family planning. Population studies, 29:127-142(1975).
16. Phillips, D.L. Abandoning method. San Francisco, Jossey-Bass, 1973.
17. In one study of TBAs in India, a questionnaire was produced, but it was
18.
abandoned when it became apparent that the constraints of a standard format ~tended to elicit stereotyped responses", As an alternative, each TBA was interviewed on the subjects of interest for between half an hour and 45 minutes, Each interview was tape-recorded. The tapes were transcribed in English, but local terms and idioms were retained. The investigators intended to use them for the preparation of a glossary of medical terms at a later date (personal communication, Dr Carl Taylor, 1977).
Oppenheim, A.N. Questionnaire design and attitude measurement. London, Heinemann, 1970,
19. The following are some reasons why it might be feasible to focus first on existing TBAs rather than on potential TBAs as candidates for training:
(a) Because existing TBAs are familiar with the work, it might be less time-consuming to help them to replace harmful practices with safe ones than it would be to train from scratch personnel who have had no previous experience in the work concerned.
(b) TBAs who are not given an opportunity of training might well form a pocket of resistance that could jeopardize the training programme and make life difficult for the new practitioners emanating from the training programme,
(c) The community may be more willing to accept new modes of practice from TBAs who have been serving the community than from new recruits, however well trained.

20.
21.
~ 96 -
(d) Information would need to be obtained on potential new recruits, since the inventory discussed earlier would cover only TBAs actually practising.
WHO Technical Report Series, No. 608, 1977 (Evaluation of learning objectives in the education of health personnel: Report of a WHO Study Group).
The following are among matters that those responsible for specifying learning objectives might profitably discuss with TBAs in order to assess more accurately their needs for learning:
which aspects of their health work they like best and which least, and why;
which aspects they find most difficult, and why;
in which tasks (procedures, techniques) they would like to improve their performance, and in which tasks they feel their clients would like them to improve their performance;
what types of health work they would like to undertake that they are not currently undertaking;
what kinds of knowledge, skills, materials, and/or equipment they feel would help them to do a better job or facilitate their work;
to whom they go for help in difficult situations connected with their health work;
what aspects of the work they feel will be the most difficult and the least difficult to learn about, and why; and
what specific to~ics they would like the training programme to cover.
22. WHO Consultation on the Role of the Traditional Birth Attendant in Maternal and Child Health and Family Planning, Geneva, 1973. Conclusions and recommendations (unpublished document).
23. Guilbert, J.-J. Educational handbook for health personnel. Geneva, World Health Organization, 1977 (WHO Offset Publication, No. 35).
24, Other considerations to be taken into account in the development of a training programme include the following:
(a) What is the period of time over which the training programme as a whole will be conducted relative to the total number of persons to be trained and the number of trainees available? These will provide a basis for determining the number and size of classes over the total programme period,

- 97 -
(b) How often, when, and for how long can participants make themselves a~~ilabie f6r training? Since most trainees may have families to look after and/or other work, e,g., in the fields, their time for training in terms of when and for how long will not be very flexible. TBA.s should be consulted about the best time for classes, the number of sessions each week, and the length of each session.
(c) What are the workload and time schedules of the trainers? Most trainers will have other ta~k~, either in the health service system or outside it, and these will have to be accommodated.
(d) How great are the distances generally separating the regular work site of the trainers from the home site of the trainees?- This factor will provide an indication of transport requirements in terms of time and mode, for trainers and/or trainees. The icieal place to conduct training would be the villages where the TBA.s live and work. Consideration should thus be given to the feasibility of having teachers go to certain villages to give courses to small groups of TBA.s who are within walking distance of the site chosen for holding classes. If, however, the TBA.s are to be brought to a health centre for the duration of the course, questions arise as to what housing facilities will be required and available, and whether candidates will require a stipend to help them with their expenses while away from home.
(e) How often and for how long are training facilities available, either at the'bealth centre or in the village?
(f) What fl!nds are available for materials, transport, food, stipends, etc. that may be needed for the programme?
(g) If training is to be conducted in the village, what equipment and supplies are available locally, either in the homes of the villagers or in the local market? If trainees are to be given kits, equipment and supplies of the nature contained therein should. be .used in teaching.
(h) What teaching aids would be the most suitable? Simple aids such as posters, diagrams, flip-charts, and flannelgraphs can be as effective as sophisticated audiovisual equfpment and may be more feasible in rural areas. Films and slide projectors, for example, require electricity, which may be lacking in certain rural areas. Moreover, existing films or slide tapes may be inimical to the culture of the locality.
(i) How will the age and literacy level of the trainees affect the content and the length of the programme, the length of teaching sessions, and the teaching and learning strategies to be used? The majority of TBA.s are older women and, in many countries, most are illiterate. The extent of their general education will determine the depth of theoretical instruction that is feasible. Certain fundamental concepts can be taught, however, provided they are presented in terms the learner can understand. With older TBAs, it may be.wise to hold short teaching/learning sessions_ interspersed with a variety of activities in which the trainees participate, e.g., group discussions_, return _demonstration, and role play.

- 98 -
(j) Are there language barriers that need to be considered? In countries where the spoken language varies from one part of the country to another, it will be essential to ensure that trainers are versed in -and can use in their training - the vernacular of the particular communities from which the trainees in their charge derive.
(k) If certificates and/or kits are to be awarded at the end of the course, will they be awarded to all who attend the course or only to those who show evidence of having mastered the course content? If the latter, what evaluation techniques will be used? In this regard, questioning, return demonstration, and role playing may be the most appropriate and effective. The question also arises as to what will happen to those who have not demonstrated the necessary learning? Should they be encouraged to try again at a later date? Should they be discouraged from practising? Perhaps it would be best to grant them the certificate and/or kit, in the hope that, through supervision, their learning will improve. Supervisors will need to be ale.rted to such cases and to the problems involved. The granting of awards should, if possible, be an occasion in which people from the TBA's home village can participate, so that they too can share in the feeling of accomplishment by one of their members. While the trainers - during the time they participated in the planning of the training programme - will presumably have familiarized themselves with the trainees' communities, it is important that, just prior to the implementation of the programme, they should be given the opportunity to meet again with village leaders and with the TBAs who will be coming to class, in order to inform them about deatils of the programme, to answer questions, and to solve unforeseen problems. If the supervisor of the TBAs is a person other than the trainer, this might be an appropriate occasion for her also to meet with the village leaders and the TBAs.
25. Thorndike, R.L. & Hagen, E.P. Measurement and evaluation in psychology and education, 3rd ed. New York, Wiley, 1969.
26. World Health Organization. The primary health worker, Geneva, 1977.
27. Fig. 8 and 9 were developed on the basis of unpublished materials supplied by Miss Hannah Mitchell, 895 Amsterdam Avenue, N.W., Atlanta, GA 30306, USA.
28. The test presented in Fig. 10 is drawn from unpublished material supplied by Dr Felipe Garc{a Sanchez, Instituto Mexicano del Securo Social, Mexico City.
29; Republic of the Philippines, Department of Health, Division of Maternal and Child Health. The good hilot helps the mother in her barrio. This brochure was prepared in a way that will make it easy for a nurse or midwife working in a rural area to reproduce copies by tracing where other

- 99 -
forms of duplication are unavailable. The following is another profusely illustrated manual: State of Alaska, Department of Health and Social Services. Division of Public Health, Sections of Nursing and Family Health. Manual for Alaska's midwives and midwifery teaching guide for public health nurses. Juneau, 1966.
30. Peng, J.Y. Village midwives deliver. IDRC Reports (Ottawa),
31.
6 (No. 2): 8 (1977).
UNICEF-WHO Joint Committee on Health Policy. Community involvement in primary health care: a study of community motivation and continued participation. (Document JC21/UNICEF-WH0/77.2). Each of the 13 rural maternity centres established by 1977 in Thies, Senegal, comprises a set of traditional huts built and equipped with the help of the villagers. Among the 2335 births that had taken place in the centres between March 1970 (when they started operating) and the time when the above-mentioned report was written, only 3 cases of neonatal tetanus had occurred. According to the report, it was concern at the high rate of tetanus in the region (50% of all perinatal deaths) that helped to promote support for the first training programme for TBA.sin the area.
32. Araujo, G. et al. Rural and semi-urban maternal-infant health programme. (Unpublished paper, 1977.) As part of a programme to achieve maximum use of local resources, with professional staff providing supervision only, volunteers in the town of Pacatuba, Brazil, were encouraged to renovate a derelict building and turn it into a maternity clinic to be staffed by trained TBA.sin rotation. A total of 30 local TBAs were sent, in groups of 6 or 8, to a teaching hospital for 3 months for intensive training in obstetrical examination and delivery, sterilization and general cleanliness, and recognition of high-risk patients. After training, the TBAs returned to their rural areas. The more skilled among them were appointed to the permanent staff of the maternity clinic. The other TBA.shave been contributing 2 days of service per month "to keep them in contact with the clinic and proper sanitary procedures". The TBAs set up and run daily clinics for prenatal, postpartum, neonatal, and paediatric care under the periodic supervision of registered nurses and physicians. Over 90% of pregnant women in the area served by the clinic have been registered there for prenatal attention and have received antitetanus vaccine. Among all the children 4 years old or younger, 98% have received DPT immunization, 81% have received poliomyelitis vaccine, and 35% have received measles vaccine. All children attending the clinic receive periodic treatment for worms. TBAs in the clinic have conducted an average of 50 normal deliveries per month over a two-year period. The report states that so far there have been no cases of infection. All high-risk patients and premature delive~ies are sent to hospital. All records are kept by TBAs. Two other clinics have been established on similar lines.
33. Costa Rica. Ministerio de Salubrided Publica, Departamento Materno-Infantil. Carnet de parteras empiricas. This document, which consists only of a variety of forms, is part of a set of unpublished documents,one of which describes the rules and regulations governing the practice of TBA.sin Costa

- 100 -
Rica. Another is a manual for TBAs (Manual para parteras emp!ricas de Costa Rica, prepared by Doris Sol<'.irzano Saborio, Haydee Gomez de Badilla, and Rosita Villegas de Guill~n, 1966).
34. With respect to transport and communications, the questions that planners need to consider include the following:
(a) What is the principa-1 mode of transport in the geographical area concerned? Do most people get around on animals or on foot? Are other means of transport available, e.g., bicycles, boats, motorized vehicles?
(b) Are the roads or tracks in reasonably good condition? Are they impassable at certain times of the year?
(c) How long does it take, under normal conditions, to get from the village to the nearest health centre and to the nearest hospital (by whatever means of transport is available)?
(d) Does the rural (or 16cal) health centre have transport facilities, e.g., a vehicle provided by the ministry of heal.th?
(e) How are messages conveyed? Are there radio-telephones or other means of direct contact with the village?
35. Boamah, Opoku. Trainers' and traditional birth attendants' experiences with ... and the use of UNICEF midwifery kit, May 1976-June 1977. This report is one of a series of unpublished repo7ts concerning the Brong Ahafo Rural Integrated Development Project (BARIPED) in Ghana. The author noted, inter alia, that 6 of the 38 TBAs had not used their kits up to the time of the interview, although all 38 insisted that the kit helped them to assist in deliveries much more efficiently and hygienically. Among those who had not yet used their kits, one said:. "I conduct _deliveries together with another TBA and we use only her kit". Another stated: "I was first go:i.~g to examine. the lady before taking_ the kit, but. when I got ther,e the time was due for her to deliver and I could not go back for the kit." A tabulation of the responses. of TBAs individually showed that only 2 of them had found all items easy to handle, while 5 had forgotten the intended use of 8 or more of the 18 items in the kit. Cne stated that she had used the towel as a cover for the kit. Because of the presence of cotton wool in the kit, some TBAs could not .remember the function of the gauze pad. Some insisted that certain items were not used during the training period and that, for this reason, they did not "remember!' their use. From the table on the following page, itmay be seen that among the items whose use was most often forgotten were solutions (mentholated spirit and disinfectant) and the dropping~bottle. The item found to be most difficult to handle was the forceps. The findings shown in the table may be useful to trainers because it shows the possible weaknesses of the training as regards the kit.

- 101 -
Table summarizing reactions of TBAs (expressed in both absolute numbers and percentages of TBAs) to the various items in the UNICEF kit
Code: E "' D
Easy to handle the item Difficult to handle the item
F Forgot or does not know the use of the item
Item
Scissors Soap Sponge bowl Kidney basin Cord ligature Mentholated spirit Plastic sheeting Cotton wool Towels Dropping-bottle Disinfectant Apron Gauze Stethoscope Cord powder Eye lotion Brush Forceps
E
No, (%)
38 (100)
3 7 ( 97) 29 (76) 34 ( 89)
36 ( 95)
16 ( 42)
34 ( 89)
34 ( 89)
27 ( 71)
7 ( 18)
23 ( 60)
37 (97) 20 (53)
30 (79) 30 (79) 33 ( 87)
36 ( 95)
10 ( 26)
Reaction
D F
No. (%) No. (%)
4 ( 11)
1 (3)
26 ( 68)
1 ( 3)
9 (24)
3 ( 8)
2 (5)
22 ( 58)
3 ( 8)
4 ( 11)
9 (24)
31 ( 82)
13 ( 34)
l ( 3)
17 ( 44)
2 ( 5)
6 (16)
5 (13)
2 ( 5) l ( 3)
No. (%) No. (%)
l ( 3)
l ( 3)
l ( 3)
2 ( 5)
l ( 3)
l ( 3)
1 ( 3) l ( 3)
36. Unpublished data from the study in Bolivia were supplied by Senora Nelly Farfan de Guillen. The information was gathered from 57 trained TBAs in Bolivia and covered the periods January-December 1976 and January-April 1977. Data concerned the numbers of births attended, women with difficult pregnancies referred to the health service, postpartum cases referred to the health service, recently born babies referred to the health service, and recent births registered at the registration office.

- 102 -
37. A study of the services provided during the first half of 1976 by 950 trained TBAs in 13 states of Mexico showed the following incidence of specified activities:
Births. attended Pregnancies attended Postnatal cases attended Other assistance given Health promotion activities Sanitation activities Hygiene education provided Cases referred for consultation Collaboration in vaccination campaigns Collaboration in other programmes Collaboration in mobile brigades Notified cases Married couples referred to family planning
programmes
Source: Dr Felipe Garcia Sanchez (see note 28).
12489 7808 8286 1345 2808 4621 8140 5842 1251 1291
98 369
2624
38. Essex, B.J. & Everett, V.J. Ese of an action-oriented record card for
39.
antenatal screening. Tropical doctor, l= 134-138 (1977). Out of a total of 13 410 women screened in antenatal clinics in Dar-es-Salaam during the study, nearly 18% were found to have one or more specified risk factors. By far the most common risk factor detected was stature. Nearly 11% of the women screened had a height of less than 146 cm. A previous study in the area had shown that one-tenth of all primigravidae of 146 cm or less in height had required a caesarian section for cephalopelvic disproportion._ Data recorded for all women during the study showed that, in the case of nearly 55% of past stillbirths and 43% of past neonatal deaths, the mother's height was under 146 cm. The authors of the report point out that the at-risk height will vary from one population group to another. It should be based on the mean height of women who have borne children in relation to that of women found to have disproportion. Presumably it would be possible to teach TBAs how to use a rod that it cut to the at-risk height and to discover basic facts about her client's past obstetric history.
World Health Organization. Risk approach for maternal and child health care: A managerial strategy to improve the coverage and quality of maternal and child health/family planning services based on the measurement of
;
individual and community risk. Geneva, World Health Organization, 1978 (WHO Offset Publication, No. 39).
40. Rogers, E.M. & Solomon, D.S. Traditional midwives as family planning communicators in Asia. Honolulu, East-West Communication Institute, 1975.
41. Poerwodihardjo,Soebagjo et al. The role of the traditional midwife in the family planning programme. Report of a national workshop related to MCH care and family planning. Jakarta, National Family Coordination Board, 1972.

- 103 -
42, Rogers, E.M. & Solomon, D.S. op.cit. (see note 40). In Malaysia, TBAs have not been permitted to dispense the initial supply of oral contraceptives but have been encouraged to act as the source of monthly supplies for women during a period of six months after their first visit to the family planning clinic and between subsequent visits. A re-supply card for each monthly cycle of pills is completed by the TBA or, on her behalf, by someone literate. According to the authors, about 77% of those who adopted oral pills were still using them after 12 months - an unusually high rate of continuation for Asian nations.
43. Simons, John. Unpublished data from a study of TBAs in Central Java, 1972. Below are data showing the distribution, by family size (number of living children), of women referred by three groups of TBAs. The referrals by groups A and C occurred over a period of two months and those by group B over four months. Groups A and B had received special training, and the subsequent work of group A was supervised. Group Chad received neither special training nor supervision.
Group of TBAs Women referred
Total No.(%)
%, by No. of living children 0 1-3 4-6 7-9 9+
A. Trained and supervised group 160 (100) 1.9 48.1 40.0 8.1 1.9
B. Trained but unsupervised group 147 (100) o.o 40.l 48.3 10.9 0.7
c. Untrained and unsupervised group 54 (100) 0.0 57.4 35.2 7.4 0.0
All groups 361 (100) 0.8 46.3 42.7 9.1 1.1
For all groups, women with relatively large families constituted a substantial proportion of the referrals. The mean family size of women referred by these groups TBAs and another group not included in the table was 3.9.
44, Tietze, C, Maternal mortality excluding abortion mortality. World health statistics report, 30, No. 4, 1977.
45. Bayoumi, A. The training and activity of village midwives in the Sudan. Tropical doctor, 6: 118-125 (1976). Between 1950 and 1975, 3889 young women from rural areas had received training in midwifery through a series of nine-month courses in a number of schools (16 in 1974) established in provincial centres in the Sudan. In the Province of Khartoum, the rate of maternal mortality, excluding mortality due to abortions, dropped to 3,2 per 1000 births in 1972. For one of the towns in that province (Omdurman) the
of

- 104 -
rate was 10,7 in 1936, The aggregate rate of 3.2 for Khartoum Province reflects a rate of 4,2 for deliveries in institutions and 3.0 for domiciliary deliveries. The author states that rates such as these should be regarded with caution because the records needed for the computation of reliable rates do not exist. Between 1950 and 1969, the maternal mortality rate reported with respect to hospital confinements alone fell from 24.8 per 1000 deliveries to 8.3. The author states that these figures refer almost exclusively to cases of bad obstetric history or obstructed labour referred to hospitals by domiciliary midwives, and that the marked drop in the rate may be ascribed to a number of factors and not simply to the village midwife programme. These factors include: the growing number of qualified obstetricians, the expansion of health services, the introduction of sulfonamides and antibiotics, and the availability of banked blood at provincial hospitals. Thus, such data may be used only as crude measures of the role of village midwives as first-contact or primary midwifery workers.
46. Chen, L.C, et al. Maternal mortality in rural Bangladesh, Studies in family planning, 5: 334-341 (1974). This is a report of two special enquiries into maternal mortality in rural Bangladesh. In the first study, conducted between 1 December 1967 and 30 November 1968, a public health obstetrician and a public health physician personally investigated all reported deaths of females of reproductive age, within 2-6 weeks of each death. A diagnosis of the probable cause of death was made on the basis of responses of family members and others to questions about signs and symptoms, A death was classified as maternity-related if it occurred when the woman was pregnant or within 40 days of the termination of pregnancy. It was found that, during this field study, which covered a total population of 115 735 and lasted one year, there were 41 deaths (30% of all deaths of women in the age range 10-49 years) that were classifiable as maternityrelated, During the same period, there were 5329 live births. The maternal mortality rate was therefore 7,7 per 1000 livebirths, Of the 41 maternityrelated deaths, 33 (over 80%) were attributed to direct obstetric causes, with eclampsia as the most common cause.
The second study included an analysis of the records of all births and deaths registered for a total population of 462 385 over the two-year period 1 May 1968 - 30 April 1970. Maternal mortality was identified by matching adult death records with reports of births and fetal deaths. Again, a death was classified as maternity-related if it occurred within 90 days of a birth or fetal death, or if the report stated that the woman was pregnant at the time of death, A total of 119 deaths of women (27% of all deaths of women in the age range 10-49 years) were found to be classifiable as maternity-related. During the period, there were 20 816 live births, giving a maternal mortality rate of 5.7 per 1000 livebirths. This rate, like that established by the first study, was substantially lower than the estimated rates for Bangladesh.
The data of the second study were analysed to discover relationships between maternal mortality and previous pregnancies. Among the 91 women with known pregnancy histories, 35 were primigravidae. Previous pregnancy losses for the remaining 56 women were substantial: they had had 292 pregnancies but

- 105 -
had produced only 169 living children, The authors point out that, because the figures were obtained retrospectively, they undoubtedly give an underestimate of the actual reproductive losses. Of the current pregnancies (those during or after which the mother died) only 49 resulted in a livebirth, 28 were undelivered, and 42 were fetal losses or stillbirths. Of the 49 liveborn children, 43 died within two months and less than 5% survived the age of one year, The risk of dying was highest for women experiencing their first pregnancy. For them, the mortality rate was 12.7 per 1000, The rate fell sharply, to about 2.5 per 1000, for women who had experienced between 1 and 3 previous pregnancies, but started to climb for women with 4 or more previous pregnancies, reaching a sustained high level of around 7 per 1000 for women with 6 or more pregnancies.
An important feature of these studies is their empirical validation of the definition of maternity-related deaths recommended by the Committee on Maternal and Child Care of the American Medical Association - i.e., deaths occurring "while the woman was pregnant or within 90 days of the termination of the pregnancy ±rrespective of the duration of the pregnancy at the time of .termination or the method by which it was terminated", The field study demonstrated that about 90% of maternal deaths fulfilling this definition were either directly or indirectly related to the process of childbearing. The authors point out that the definition might be very useful in other situations where information on the cause of death is lacking.
Discussing policy implications, the authors say .. that antenatal heal th services might prevent most- cases of eclampsia, potentially reducing the mortality rate a~ong primigravidae by about 75% and maternal mortality by about 30%. However, they point out that a considerable investment in ·health services would be required to achieve this result, since 99 of 100 primigravidae are not at risk of this complication. They go on to say that, while some causes of maternal mortality, such as postpartum tetanus, might be prevented by simple instructions in the management of home deliveries, "it is evident ••• that at least a third of maternal deaths are due to complications of pregnancy requiring more sophisticated facilities for anesthesia, surgery, and blood transfusions". Their own prescription is a "vigorous and well-directed family planning programme" which, they believe, might reduce maternal mortality by reducing risks associated with large families and rapidly recurring pregnancies.
47. Vallin, J, World trends in infant mortality since 1950, World health statistics report, 29: 646-674 (1976).
48. Puffer, R.R. & Serrano, C.V. Patterns of mortality in childhood. Report of the Inter-American Investigation of Mortality.in Childhood, Washington, DC, Pan American Health Organization, 1973 (Scientific Publication, No. 262). The investigation was carried out in 13 widely separated areas in Latin America and 2 in North America. Of a total of 35 095 deaths of children under 5 years of age that were investigated, 12 674 occurred during the neonatal period. The following data, extracted from various tables in the report, show the distribution of neonatal deaths by underlying cause of death:

- 106 -
All causes
Perinatal causes:
Immaturity
Conditions unrelated to pregnancy
Toxaemia
Maternal infection
Premature rupture of membranes
Hydramnios
Multiple pregnancy
Other complications
Placenta praevia
Premature separation
Other conditions of placenta
Conditions of cord
Pelvic abnormality, disproportion
Malposition of fetus
Other and unspecified difficult labour
Birth injury unspecified
Fetal distress, anoxia
Aspiration of contents of birth canal
Respiratory distress
Asphyxia of newborn
Haemolytic disease of newborn
Postmaturity
Haemorrhagic disease of newborn
Other conditions of newborn
Causes other than neonatal:
Diarrhoeal disease
Other infectious diseases
Diseases of respiratory system
Congenital anomalies
Other
Ko.
12 674
440
360
334
133
550
72
815
455
305
261
24
211
127
550
475
400
206
209
1 075
657
213
4
181
74
1 269
663
1 176
881
554
l2. 100
3,47
2.84
2.63
1.04
4.34
0.57
6.43
3.59
2.41
2.06
0,19
1.66
1,00
4,34
3.75
3.16
1,62
1.65
8,48
5.18
1,68
0.03
1.43
0,58
10.01
5.23
9.28
6.95
4.37

- 107 -
The authors stress that, although excessive mortality in children is due mainly to acute morbid conditions, important contributory causes, such as low birth weight, immaturity, and nutritional deficiency, may have their origin in factors acting over long periods of time. The study revealed that immaturity is a very serious problem in many areas of Latin America. The authors regard this condition as the most important factor in vulnerability to disease and death in the neonatal period. Immaturity was assigned as either an underlying or an associated cause of death whenever either a birth weight of 2500 g or less or a clinical or pathological diagnosis of immaturity or prematurity was recorded. In 9 of the 15 areas studied, more than 60% of neonatal deaths were those of infants known to be immature. For all areas combined, immaturity was assigned as the underlying cause in 3.5% of cases, but as an associated cause (i.e., either contributing to the fatal outcome of other causes or deriving from such causes) in 57% of cases.
Immaturity and low birth weight are believed to be attributable, at least in part, to the poor nutritional state of the mother. The authors cite evidence from a study in Guatemala, which showed that the provision of additional food (20 000 calories or more during pregnancy) resulted in an increase of nearly 9% in mean birth weight. The impact of nutritional deficiency on mortality among children surviving the neonatal period turned out to be even greater than the impact of immaturity on neonatal mortality. Nutritional deficiency is assigned as the underlying or associated cause in 52% of the 21 951 deaths of children occurring after the neonatal period in the 13 Latin American areas studied.
The authors stress the importance of nutrition programmes to improve the nutritional state of the future mother and to promote the normal growth and development of the child. It is widely believed that this is an area where trained TBAs could have an impact. While this may be so, it is important to recognize that the major causes of malnutrition in mothers and their offspring are not among those which TBAs could easily influence. For example, the TBA cannot be expected to provide extra food when this is the basic requirement, or to relieve a pregnant woman of hard physical work. On the other hand, the TBA may be able to help to persuade mothers to breast-feed their babie~ for an adequate period. The study found that breast-feeding for one month or longer had been provided for only 52.5% of infants who died in the post-neonatal period. The TBA can also help to encourage more mothers to accept prenatal care, as has been demonstrated by some programmes. The study found a strong inverse correlation between the infant death rate in one area and the proportion of mothers receiving prenatal care.
49. Gordon, J.E., Gideon, H. & Wyoni J.B. Midwifery practice in rural Punjab, India. American journal of obstetrics and gynecology,~: 734-742 (1965). The study population numbered 12 022 persons in 11 villages of Punjab State, north India. Infant mortality in the area was 161.7 per 1000 livebirths. Almost half the deaths occurred within the neonatal period. Neonatal tetanus accounted for about one-quarter of neonatal deaths occurring during the study, with postnatal asphyxia and atelectasis at a similarly high level. Data were collected at the time of birth or within the ensuing month by trained health workers under the close supervision of a physician. Deaths were investigated individually by a physician. The study, which was part of a longer project, took place in the two years April 1956 to March 1958. A total of 864 births were investigated. Most of these were attended by 25 untrained TBAs. The others were attended either by four TBAs who had attended brief periods of training or by two nurse-midwives each of whom had had a combined training of 18 months in nursing and midwifery.

- 108 -
The perinatal death rate was shown to be strongly associated with prolonged labour, but, when parity and the age of the mother were taken into account, there was no significant difference in the duration of labour between the mothers attended by untrained TBAs and those attended by trained personnel. An analysis of neonatal deaths in relation to the instrument used for cutting the cord showed that neonatal death rates were the lowest and that there were no cases of tetanus when a knife was used. The apparent association of the instrument used and other factors with all neonatal deaths and with neonatal deaths from tetanus is shown in the tabulation below.
Instrument for cutting cord
Scissors
Trowel
Sickle
Knife
Unknown and others
Initial dressing of umbilical cord
Ash
Powder
Ghee
Mustard oil
Tied only
Unknown and others
Sex of child
Male
Female
Attendant at birth
Trained midwife
Untrained midwife
Other attendants
All liveborn infants
Ko, of infants
339
253
81
112
52
337
129
109
147
55
60
440
397
199
619
l9
83 7
Xo.
19
23
8
3
5
25
4
4
9
5
11
22
36
10
46
2
58
Neonatal deaths
As"; of infants
5.6
9.1
9.9
2.7
9.6
7.4
3.1
3.7
6.1
9.1
18.3
5.0
9.1
5.0
7.4
10.5
6.9
No.
5
4
3
0
0
9
0
1
0
1
1
7
5
2
10
0
12,
Neonatal deaths from tetanus
As% of infants
1.5
1.6
3.7
o.o
o.o
2.7
o.o 9.0
o.o
2.0
1.7
1. 6
1.3
1.0
1.6
o.o
1.4
As% of neonatal deaths
26.3
17.4
37.5
o.o o.o
36.0
o.o 25.0
o.o
20.0
9.1
31.8
13. 9
20.0
21. 7
o.o
20.7

50.
- 109 -
For more than half the deliveries attended by untrained midwives, the umbilical cord dressing consisted of ash from a mixture of cow dung, straw, and earth, the fuel used universally in the country for cooking and heating. By contrast, trained attendants usually used powdered talc purchased at the local pharmacy. The data above show that the use of ash was associated with the highest frequency of death from tetanus. The high death rate shown for the category "tied only" is explained by the fact that often no dressing was applied because the baby died shortly after birth,
The investigators attribute higher neonatal death rates for infants delivered by untrained midwives in part to a greater number of unduly long periods· of labour. Death rates from postnatal asphyxia and atelectasis were 28 per 1000 livebirths for untrained and 9 for trained attendants. The preferences of untrained attendants for the use of ash as a dressing and, to a lesser ex"tent, the use of unsatisfactory instruments to cut the cord were considered to be other contributory factors,
The investigators conclude that, although the major factor in infant mortality in the Punjab is death occurring after the neonatal period from causes unrelated to the obstetric procedure, the number of perinatal and neonatal deaths is of such magnitude that obstetrical management has a prominent place in any general programme aimed at improving maternal and child health. "To that end, the direction of effort is seemingly to amplify and extend facilities for instruction of village midwives, to use the better trained nurse-midwife in a supervisory capacity where her efforts would have more effect, and to initiate a system of midwife registration. Immunization and re-immunization of expectant mothers with tetanus toxoid could restrict a main cause of death among the newborn. The fundamental need is health education, of the public and of midwives, toward bette_r appreciation of the risks to which the newborn infants are exposed, of the unnecessary costs in deaths, and the good and bad influence of existing customs, prejudices and traditional practices,"
Dibsosubroto, S., Ruskadi, M. & Ashali, M.S, Attitude and knowledge of parents of neonates admitted with tetanus neonatorum, Paediatrica Indonesiana, ~: 67-74 (1978).


















