Music Therapy Today Vol. VII (3) (October) 623 Traditional oriental music therapy – a regulatory and relational approach Gerhard Tucek Introduction Traditional oriental music therapy is a system documented over about one thousand years, of therapeutic, prophylactic and rehabilitative rele- vance, as we see it today, and has proved its worth in practice. In its tradi- tional form it was used in hospitals as a regular paramedical discipline and part of Islamic arts of healing from the 9th century onwards. One theoretical basis was humoral pathology (the theory of four humours), another the religious-philosophical conviction that music – as an audible musical transposition of cosmic sound – nurtures the „spirit soul“ as well as the „material body“. The idea was that a variety of different microtonal scales (Makamat) helped to produce certain desired effects in organic systems and emotions through a regulative effect of music on the „humours“. For further his- toric details see references 1 .
Transcript
Music Therapy TodayVol. VII (3) (October)
Traditional oriental music therapy – a regulatory and relational approach
Gerhard Tucek
Introduction
Traditional oriental music therapy is a system documented over about
one thousand years, of therapeutic, prophylactic and rehabilitative rele-
vance, as we see it today, and has proved its worth in practice. In its tradi-
tional form it was used in hospitals as a regular paramedical discipline
and part of Islamic arts of healing from the 9th century onwards.
One theoretical basis was humoral pathology (the theory of four
humours), another the religious-philosophical conviction that music – as
an audible musical transposition of cosmic sound – nurtures the „spirit
soul“ as well as the „material body“.
The idea was that a variety of different microtonal scales (Makamat)
helped to produce certain desired effects in organic systems and emotions
through a regulative effect of music on the „humours“. For further his-
toric details see references1.
623
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today
(Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
With the replacement of the humoral-pathological treatment model by
the concept of biomedicine, this therapy approach disappeared from hos-
pitals in Turkey and the Arab countries. In the middle of the 1980s, Oruc
Güvenc returned to the approach in Istambul and tried to re-establish it in
the traditional form. His efforts assumed an intercultural dimension
through cooperation with this author from 1984 onwards (compare
Tucek, 2003). In Austria today, the approach has been adapted to local
conditions with regard to clinical needs, is well established and increas-
ingly evaluated according to scientific criteria (see below).
A basic difference between the traditional and the current therapy con-
cept may be summed up as follows: in the Middle Ages, music was inter-
preted as an objective quality of being (in orient and occident alike). The
individual was able to make this quality visible, but not capable of pro-
ducing it himself.
Today, in contrast, music is interpreted as a subjective human expression
that may find its fulfilment in beauty.
For an understanding of traditional oriental music therapy (as it is prac-
ticed and taught in Austria today) this change means that the therapeutic
effects are no longer based on a ‚cosmic system’ from outside, but rather
on a re-structuring of an inner system. This occurs in the work (by those
involved in the process) on meaningful musical contents and forms of
expression that may be experienced as pertinent. The method used in this
context comprises an alternating musical dialogue between patient and
therapist (compare Tucek 2005a), the „regulative-medical“ effects of
music played live by the therapist, as well as therapeutic movement and
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today
(Online
1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
An essential challenge to traditional oriental music therapy (as part of
the cultural transfer) was a scientific analysis of the receptive method in
regard of the theory of an organ and emotion specific effect of the
Makam structures.
Against the background of modern brain research findings that under-
stand the brain as a socio-cultural organ1, the theory of a transferability
of specific emotional influences through Arab or Muslim musical styles
on a European patient must be doubted.This is due not so much to any
cultural prejudices but rather to culturally influenced (sound) preferences
and images (on the part of therapist and patient).
Nevertheless, clinical practice of traditional oriental music therapy shows
clearly documented therapeutic effects.
Some remarks in this context from the perspective of cultural and social
anthropology:
Man is a universal and at the same time a culture-specific being with
regard to music perception.
• A universally human level is the location for the psycho-physiologi-cal effects of rhythms (drums, rattles, etc.) and sound spaces (har-monic overtone singing, gong, etc.)
• The level of culturally shared experience with pertinent associations may be illustrated with the following example: most people in our cul-ture associate the Christmas carol „Stille Nacht, heilige Nacht / silent night, holy night“ with a festive or joyful mood.
• Let us now imagine a family singing this song in front of the illumi-nated Christmas tree when the father breaks down with a heart attack and dies. We may assume that what this song will evoke in this partic-ular family in future will not be a festive mood but grief (level of sub-jective experience).
1. Apart fro the genetic foundation, human experience is influenced by a multitude of „epigenetic“ factors (cultural, social, individual experience context).
Introduction 625
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today
(Online
1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
On the understanding that the therapist has incorporated the oriental
musical material thoroughly in the course of his training and supervised
practice, then he might be able to transfer basic emotional moods like joy,
calm, peace etc. through a loving and joyful therapeutic relationship in
support of the music.
It is possible to establish new, and for the patient positive, sound experi-
ences in this way (via Makam scales and oriental instruments). In select-
ing the modes and pieces of music, however, we must ensure that the
chosen musical structures are not too remote from what a patient is used
to listen to.
In simple words, we must find a way between a potential „fascination“
for what is new, and a potential rejection of what is „just too strange“. If
the therapist is successful here, he will stimulate therapeutic processes in
the patient the physiological correlates of which may be measured and
illustrated chronobiologically.
A superior objective of the therapy is the intention to support patients
during therapy in recovering a harmonic interplay between external cul-
tural life style and internal subjective harmony.
In this sense,
“… music is not only what it is, it is what it means to the individ-ual, what it can do for him or her … the pursuit of music can show human beings what they have in common.” (Sir Simon Rat-tle)
Hesse demonstrated that a subjective access to various types of music in
the course of a human life is not static but changes continuously (2003,
p.7).
Introduction 626
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today
(Online
1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
In addition, our subjective access to music is determined by external fac-
tors. In our clinical practice we frequently observed patients and their
families who developed a very positive attitude to musical offers of
receptive traditional oriental music therapy; but after release from hospi-
tal they did not continue. Only upon re-hospitalization did this type of
music regain significance. Therefore, a positive response to traditional
oriental music seems to be conntected to the clinical setting. A relative
said: “Now that I am back among the group, I know what I have been
missing for the last six months.” Music thus serves to recreate the mood,
not only as recreation, but as a turn to the innermost core. On this basis,
music provides a natural foundation for the recovery of the “entire self”,
even if the individual is seen as “sick” or “handicapped” in the medical
sense.
I believe an important effect of traditional oriental music therapy is that
in first contact there are no (previously) established individual associa-
tions with known musical styles, since the sound (instruments, Makam
structure) is so new and different. This leaves room for new structures
and new associations.
Music therapy in medicine / music medicine
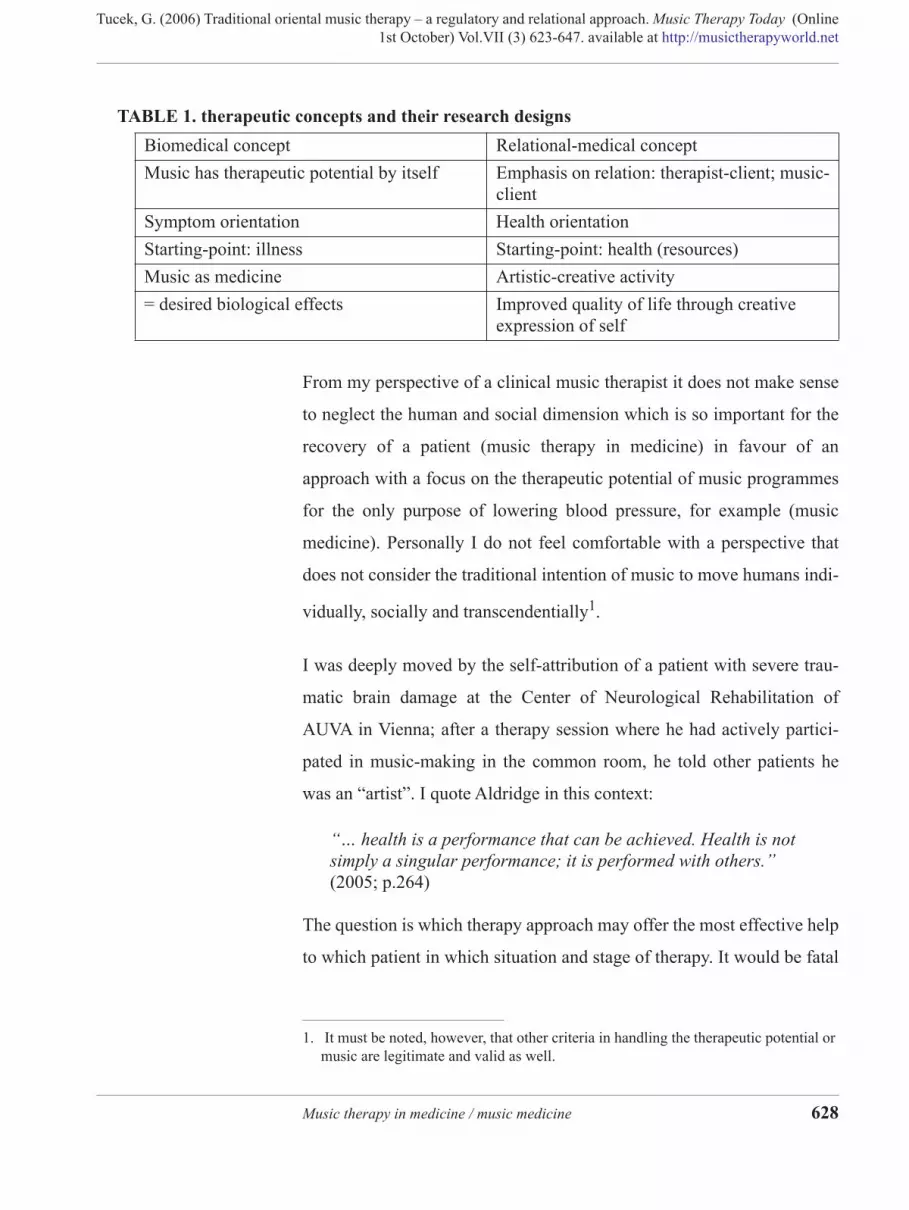
I want to give a short description of the relationship between “music
medicine” and “music therapy in medicine”. The following table by
Krautschik (2003) sums up the most important positions which have con-
siderable influence on the respective therapeutic concepts and their
research designs.
TABLE 1. therapeutic concepts and their research designs
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today
(Online
1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
From my perspective of a clinical music therapist it does not make sense
to neglect the human and social dimension which is so important for the
recovery of a patient (music therapy in medicine) in favour of an
approach with a focus on the therapeutic potential of music programmes
for the only purpose of lowering blood pressure, for example (music
medicine). Personally I do not feel comfortable with a perspective that
does not consider the traditional intention of music to move humans indi-
vidually, socially and transcendentially1.
I was deeply moved by the self-attribution of a patient with severe trau-
matic brain damage at the Center of Neurological Rehabilitation of
AUVA in Vienna; after a therapy session where he had actively partici-
pated in music-making in the common room, he told other patients he
was an “artist”. I quote Aldridge in this context:
“… health is a performance that can be achieved. Health is not simply a singular performance; it is performed with others.” (2005; p.264)
The question is which therapy approach may offer the most effective help
to which patient in which situation and stage of therapy. It would be fatal
Biomedical concept Relational-medical concept
Music has therapeutic potential by itself Emphasis on relation: therapist-client; music-client
Symptom orientation Health orientation
Starting-point: illness Starting-point: health (resources)
Music as medicine Artistic-creative activity
= desired biological effects Improved quality of life through creative expression of self
TABLE 1. therapeutic concepts and their research designs
1. It must be noted, however, that other criteria in handling the therapeutic potential or music are legitimate and valid as well.
Music therapy in medicine / music medicine 628
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today
(Online
1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
to replace positions of music therapists by musical programmes in future
in order to save money.
From empirical experience to scientific foundation:
The clinical variety of traditional oriental music therapy of today com-
bines both concepts in its equally “regulatory-medical” and “relational-
medical” approach. In the past, we evaluated clincial therapy processes
via empirical observations and documentation (case description, video
documentation).
In addition we intend to found this approach on physiological “hard
facts”. Early clinical studies (Murg, Tucek et al., 2002; Tucek, 2005b;
Tucek et al., 2006) represented important steps. Clinical practice, how-
ever, was full of organisational hurdles. Selected research methods often
limit the freedom of therapists to act. Consequently we continued to look
for methods that would not confine a music therapist (in the sense of a
best practice model) to a previously determined method of intervention
(active versus receptive).
Regulatory-medical concept and receptive traditional oriental music therapy
In a receptive therapy approach, precomposed pieces (comparable to the
so-called play songs in Nordoff Robbins music therapy) alternate with
rhythmically improvised passages. The effects observed were activating
and deactivating respectively (sympathicotonic versus parasympathico-
tonic).
Results of a clinical EEG study at the Meidling centre for neurological
rehabilitation on patients with severe traumatic brain damage revealed
From empirical experience to scientific foundation: 629
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today
(Online
1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
that this receptive approach may have relaxing effects (reduced spasms)
and at the same time improve vigilance (Murg, Tucek et al., 2002; Tucek
et al., 2006).
Similar relaxing and anxiolytic effects were reported in a study with 64
patients at the Groß Gerungs centre for cardiological rehabilitation
(Tucek, 2005b). A recent clinical study on in-patient treatment for
depressive episodes had comparable results (Scharinger, 2006).
In summary: Traditional oriental music therapy appears to be a well-
established means with a regulatory influence on mental-physiological
processes.
We now look at the question whether in addition to regulation (activating
/ deactivating effects) it is also possible to influence organs in a more dif-
ferentiated way. The following – simplified – aspects are taken into con-
sideration:
• If the therapeutic agent is in the structure of the note scales them-selves, then this should have a direct impact on the body in the sense of a physical resonance phenomenon. (Assumption: Makam has (physiological) effects independent of cultural imprint).
• If the therapeutic agent is in the mental influence via the associative channel, then music would be connected with previous cultural and individual experience in its predictable effects. (Assumption: All peo-ple – even all individuals – have “their own” music)
• If the therapeutic agent is in the musical relationship, then music would be a human-relational resonance phenomenon. (Assumption: music functions as a significant field of experience and activity)
Current research approach
The dimension of relational and regulatory medicine will now be illus-
trated with two examples of measurement and on the basis of different
chronobiological methods of data collection:
Current research approach 630
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today
(Online
1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
• Example 1 shows the change in the regulation state in a patient with
acute myelotic leukemia (AML)1 through music therapy.
• Example 2 illustrates the relational dimension between therapist and
patient with acute lymphatic leukemia (ALL)2 in the course of a ther-apy unit with individual synchronous stages. (compare Tucek et al., 2006)
EXAMPLE 1 A portable ECG apparatus with a scanner frequency of 4096 Hz, i.e.
many times higher than traditional long-term ECG appliances, measures
heart rhythms. The resulting so-called “spectrogram” reflects the rhythms
of numerous endogenous systems (respiration, peristalsis, hormonal
secretion etc.). The differences in the sequence of heart beats show the
respective dominance of one of the two branches of the autonomic ner-
vous system on the pacemaker nodes of the heart. (The sympaticus acts
as an accelerating part of the autonomous nervous system (ANS) and
generates fight, flight, performance etc.)
The parasympathicus in contrast supports regeneration and recovery.
This is why the parasympathically controlled part of the heart rate vari-
ability (HRV) is an indication of the ability to recover, which is an essen-
tial precondition for health.
The following health parameters may be deduced from HRV measure-
ments:
1. AML is a malignant cancer of myeloblasts. These are the immature preforms of var-ious granulocytes. The immature granulocytes are nonfunctional and divide in uncontrolled fashion. Then they suppress the healthy blood cells from blood and bone mark and often infiltrate spleen, liver and brain. AML is the most frequent form of leukemia in adults. (Reference: www.ArztScout.com, per July 13, 2006)
2. ALL develops like this: Lymphocytes (subtype of white blood cells) that are respon-sible for immune processes degenerate. Degenerated lymphatic cells collect in the bone mark, destroy growing blood cells and replace them. (Reference: www.ArztScout.com, per July 13, 2006)
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today
(Online
1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
• General condition, vitality, “biological age”: the product of constitu-tion and lifestyle. (Even with best genetic preconditions, “wasting ill-nesses” or unhealthy lifestyle may use up resources.)
• Regulatory capacity: adaptation and interaction between resonant fre-quency (day – night, rest – activity) and external influences (appoint-ments, others, sports etc.)
• Physical resilience: lower pulse in sleep, heart rate under and after stress, range and intensity of frequency analysis of heart rate sequence reflect the potential in this area.
• Mental resilience: detection at 0.1 Hz. in combination with pulse-res-piratory quotient, heart rate and variability in the respiration-modu-lated high frequency range are indicators of mental resilience.
• Ability to recover: Recovery is the basis for resilience. Sympathicus reduction and simultaneous increase in high frequency parts of heart rate variability, decrease of pulse and respiration frequency are objec-tive units of measurement.
• Quality of sleep: qualitative and quantitative aspects of calm and deep sleep phases are evaluated. Extent of vagus activity.
The coordination of respiratory frequency and heart rate sequence pro-
duces a restructuring of psycho-physiological processes in the sense of an
“economization” of the entire system that is reflected in the “spectro-
gram”.
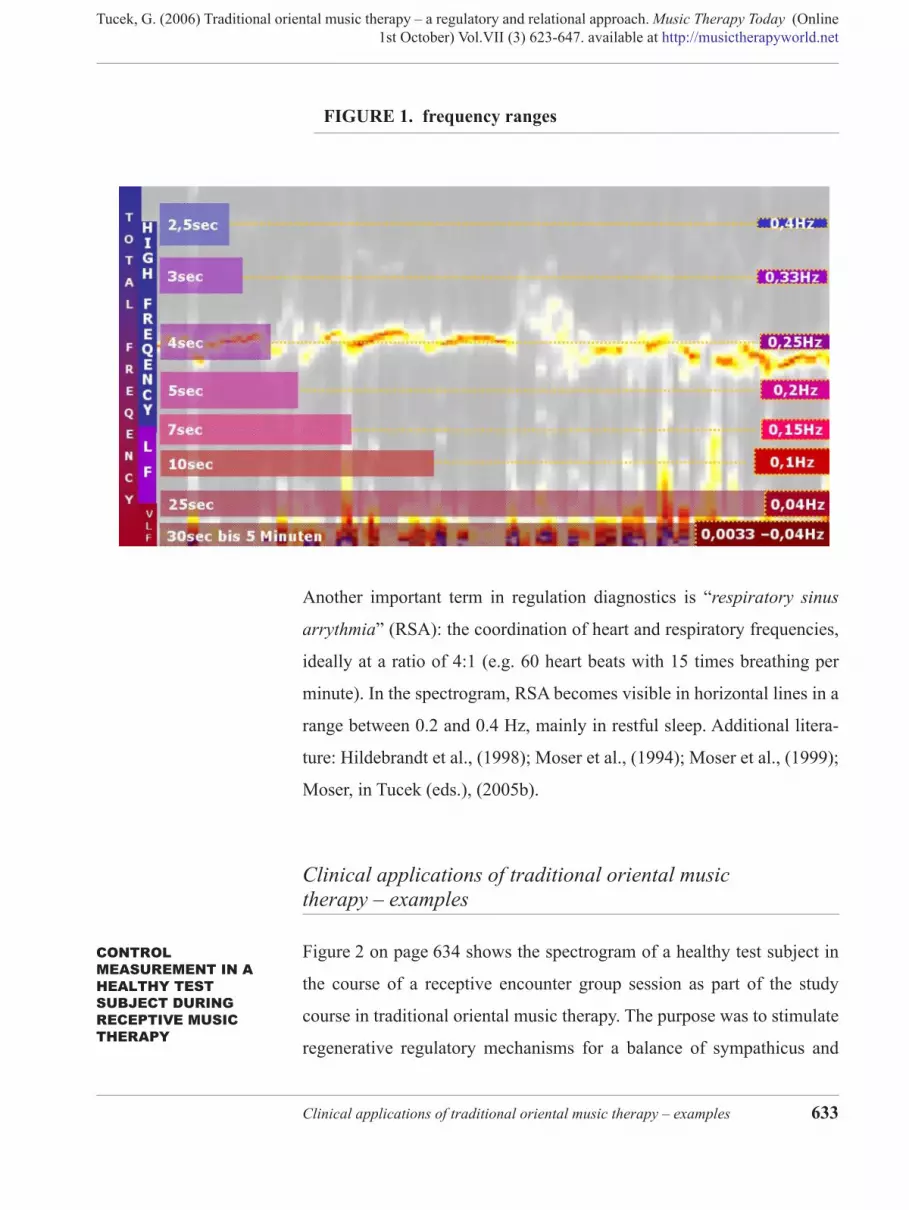
This comprises the following frequency ranges (Figure 1 on page 633):
• Very Low Frequency (VLF), a range between 25 sec. and 5 min. with a frequency of 0.04 – 0.0033 Hz., dependent on body position, physical activity and thermoregulation.
• Low Frequency (LF), a range between 7 to 25 seconds and a frequency of 0.04 and 0.15 Hz. It is parasympathically and sympathically con-trolled and corresponds to the blood pressure rhythms.
• High Frequency (HF) as presented in the figure moves between 2,5 and 7 seconds in a range of 0.15 to 0.4 Hz. It is parasympathically controlled and modulated via respiration.
Current research approach 632
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach.
Music Therapy Today (Online
1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
FIGURE 1. frequency ranges
Another important term in regulation diagnostics is “respiratory sinus
arrythmia” (RSA): the coordination of heart and respiratory frequencies,
ideally at a ratio of 4:1 (e.g. 60 heart beats with 15 times breathing per
minute). In the spectrogram, RSA becomes visible in horizontal lines in a
range between 0.2 and 0.4 Hz, mainly in restful sleep. Additional litera-
ture: Hildebrandt et al., (1998); Moser et al., (1994); Moser et al., (1999);
Moser, in Tucek (eds.), (2005b).
Clinical applications of traditional oriental music therapy – examples
CONTROL MEASUREMENT IN A HEALTHY TEST SUBJECT DURING RECEPTIVE MUSIC THERAPY
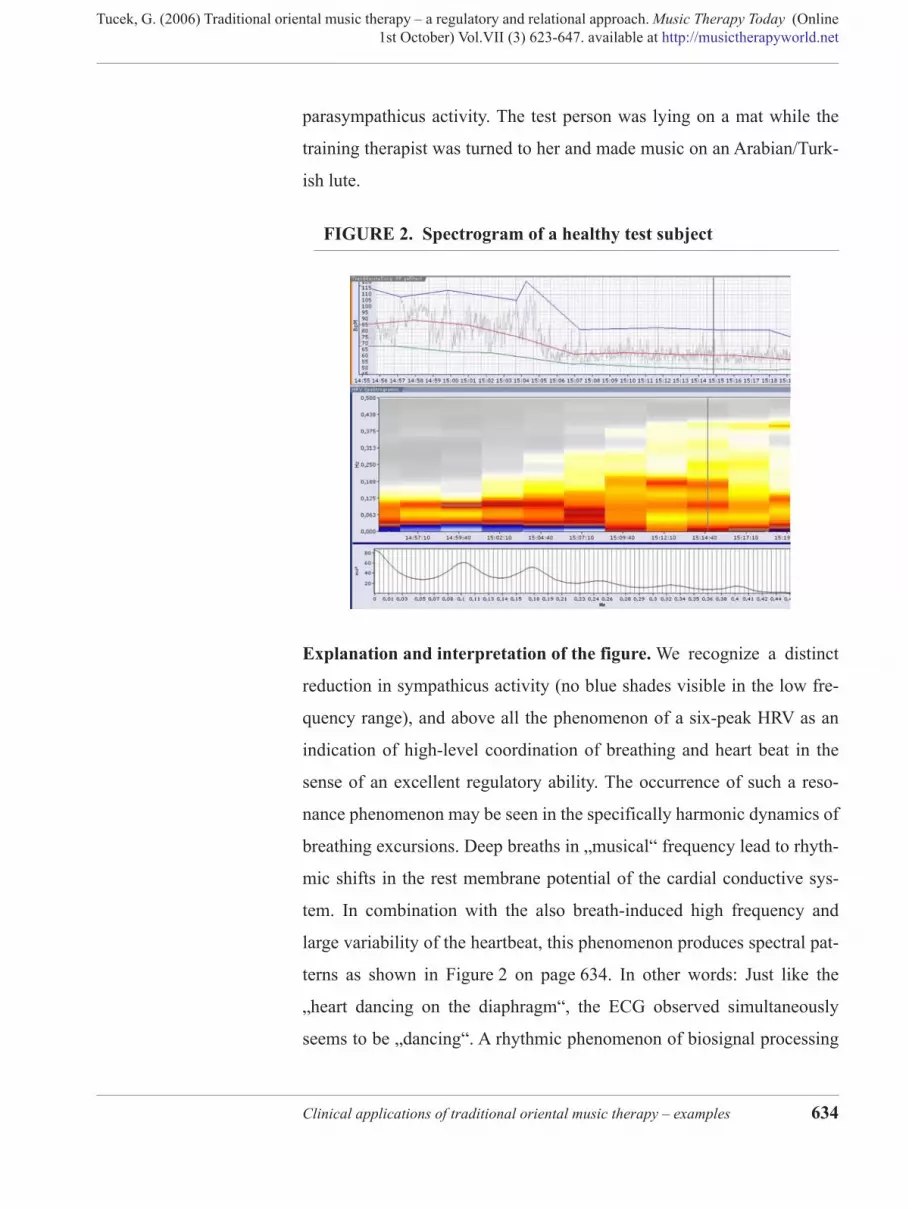
Figure 2 on page 634 shows the spectrogram of a healthy test subject in
the course of a receptive encounter group session as part of the study
course in traditional oriental music therapy. The purpose was to stimulate
regenerative regulatory mechanisms for a balance of sympathicus and
Clinical applications of traditional oriental music therapy – examples 633
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
parasympathicus activity. The test person was lying on a mat while the
training therapist was turned to her and made music on an Arabian/Turk-
ish lute.
FIGURE 2. Spectrogram of a healthy test subject
Explanation and interpretation of the figure. We recognize a distinct
reduction in sympathicus activity (no blue shades visible in the low fre-
quency range), and above all the phenomenon of a six-peak HRV as an
indication of high-level coordination of breathing and heart beat in the
sense of an excellent regulatory ability. The occurrence of such a reso-
nance phenomenon may be seen in the specifically harmonic dynamics of
breathing excursions. Deep breaths in „musical“ frequency lead to rhyth-
mic shifts in the rest membrane potential of the cardial conductive sys-
tem. In combination with the also breath-induced high frequency and
large variability of the heartbeat, this phenomenon produces spectral pat-
terns as shown in Figure 2 on page 634. In other words: Just like the
„heart dancing on the diaphragm“, the ECG observed simultaneously
seems to be „dancing“. A rhythmic phenomenon of biosignal processing
Clinical applications of traditional oriental music therapy – examples 634
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
which we also know from the analysis of heartrate variability in song and
speech therapists (compare Moser 1999), and which here also correlates
with subjective perceptions like general well-being, clarity, regeneration
etc.
The occurrence of such resonance phenomena without „indication of
breath“ via (speech) melody, rhythm, metre etc., exclusively as part of a
merely passively perceived melody, must - we assume - be based on the
interaction with the playing music therapist. The occurrence in a merely
passively received melody is unusual and not to be expected according to
previous experience with perception from audio equipment. The reason
of this resonance effect is not quite clear. We assume that the phenome-
non is due to two components, the trusting relationship (the training ther-
apist and the student knew each other) and the music (as an agent
conveying calm and relaxation)1.
An example of measurement of a healthy test subject in a traditional “healing dance” (Bakse)
The following Figure 3 on page 636 and Figure 4 on page 636 show the
spectrograms of the same test person during a traditional “Bakse” dance
used for activation (for details see Tucek 2003b).
1. Further research projects addressing this question are in preparation.
An example of measurement of a healthy test subject in a traditional “healing dance”
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
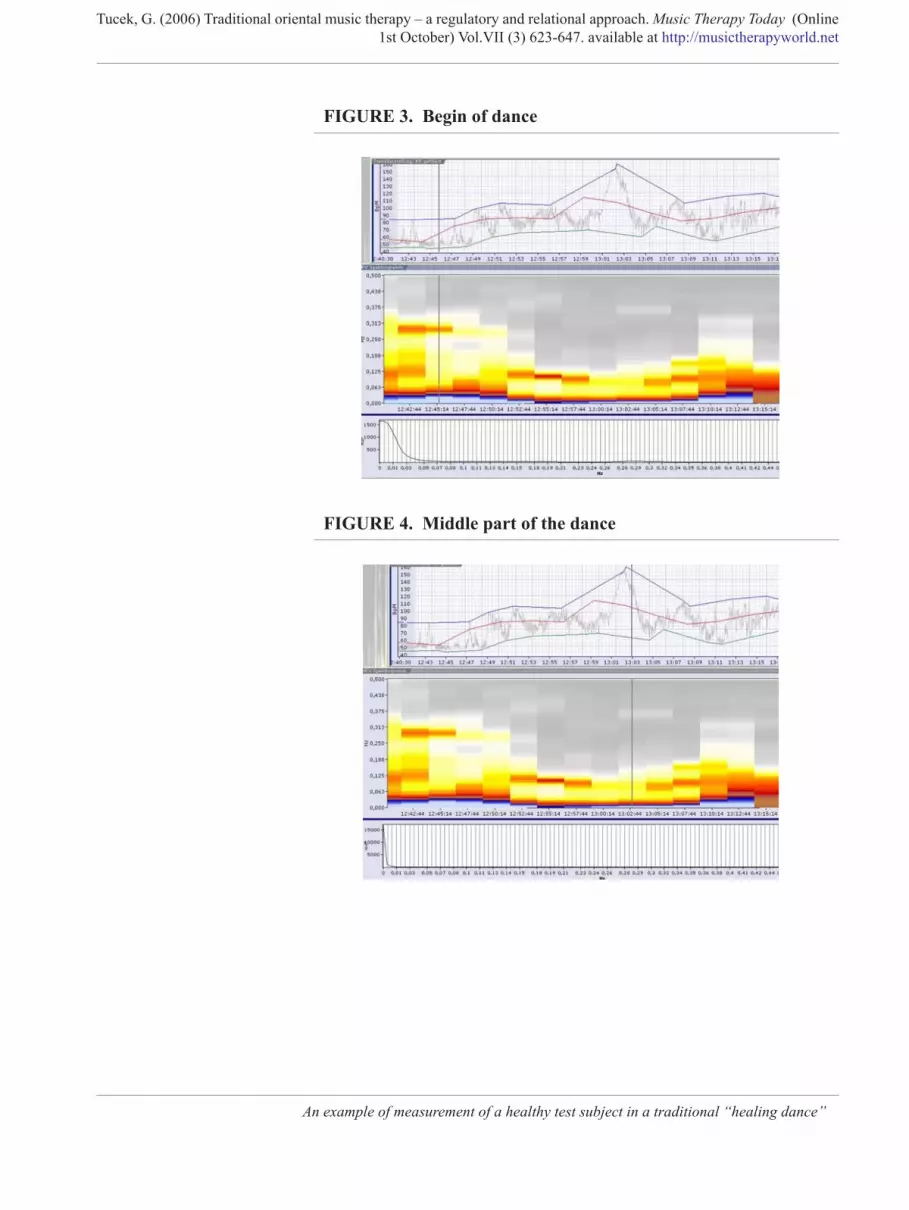
FIGURE 3. Begin of dance
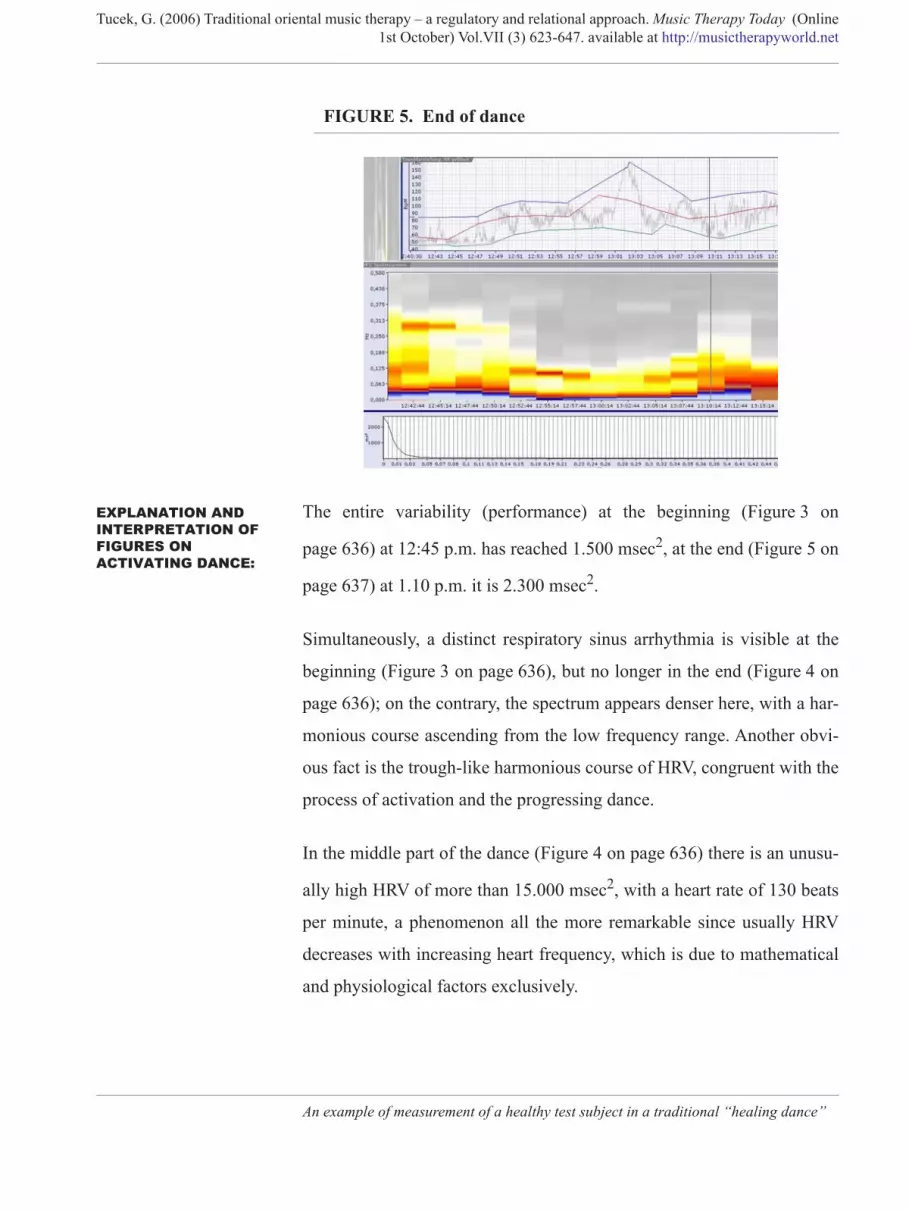
FIGURE 4. Middle part of the dance
An example of measurement of a healthy test subject in a traditional “healing dance”
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
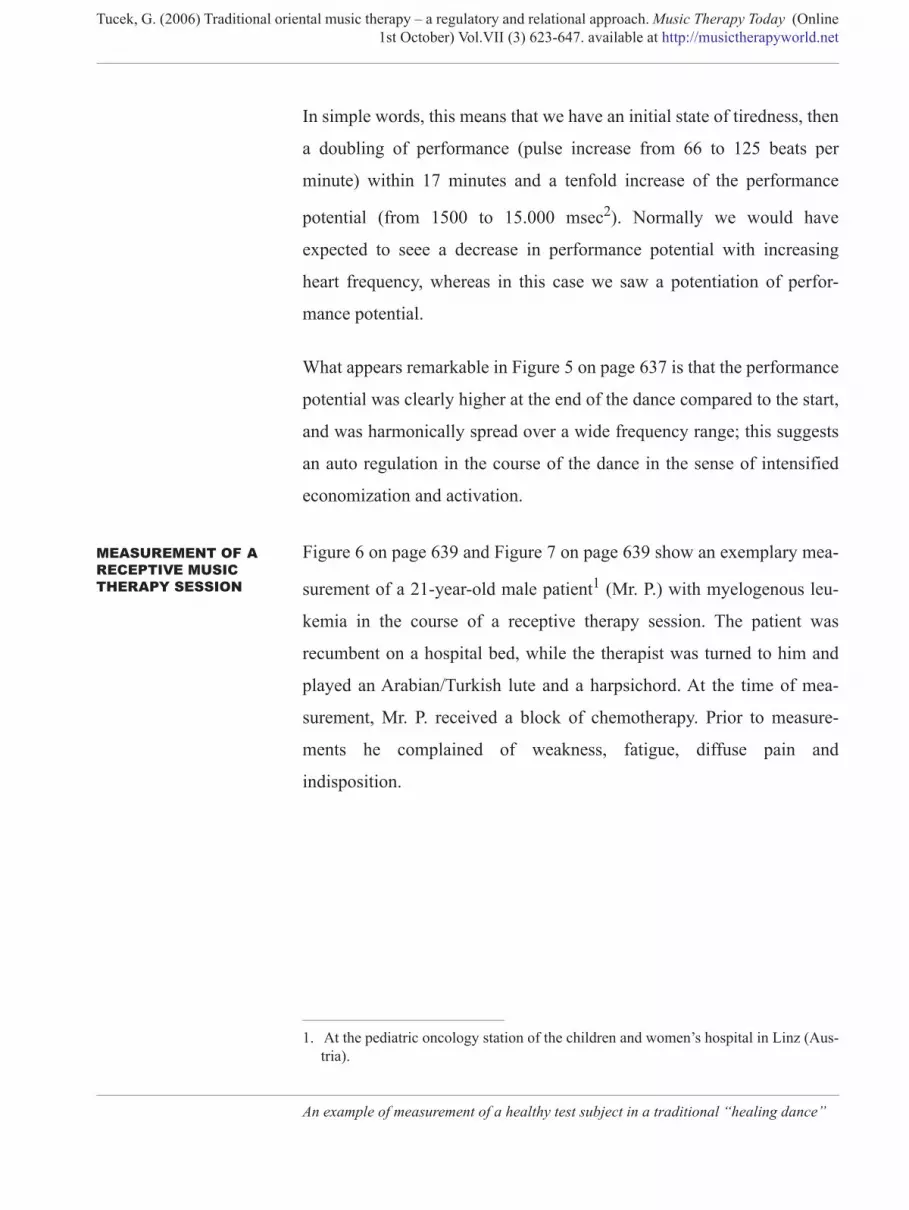
FIGURE 5. End of dance
EXPLANATION AND INTERPRETATION OF FIGURES ON ACTIVATING DANCE:
The entire variability (performance) at the beginning (Figure 3 on
page 636) at 12:45 p.m. has reached 1.500 msec2, at the end (Figure 5 on
page 637) at 1.10 p.m. it is 2.300 msec2.
Simultaneously, a distinct respiratory sinus arrhythmia is visible at the
beginning (Figure 3 on page 636), but no longer in the end (Figure 4 on
page 636); on the contrary, the spectrum appears denser here, with a har-
monious course ascending from the low frequency range. Another obvi-
ous fact is the trough-like harmonious course of HRV, congruent with the
process of activation and the progressing dance.
In the middle part of the dance (Figure 4 on page 636) there is an unusu-
ally high HRV of more than 15.000 msec2, with a heart rate of 130 beats
per minute, a phenomenon all the more remarkable since usually HRV
decreases with increasing heart frequency, which is due to mathematical
and physiological factors exclusively.
An example of measurement of a healthy test subject in a traditional “healing dance”
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
In simple words, this means that we have an initial state of tiredness, then
a doubling of performance (pulse increase from 66 to 125 beats per
minute) within 17 minutes and a tenfold increase of the performance
potential (from 1500 to 15.000 msec2). Normally we would have
expected to seee a decrease in performance potential with increasing
heart frequency, whereas in this case we saw a potentiation of perfor-
mance potential.
What appears remarkable in Figure 5 on page 637 is that the performance
potential was clearly higher at the end of the dance compared to the start,
and was harmonically spread over a wide frequency range; this suggests
an auto regulation in the course of the dance in the sense of intensified
economization and activation.
MEASUREMENT OF A RECEPTIVE MUSIC THERAPY SESSION
Figure 6 on page 639 and Figure 7 on page 639 show an exemplary mea-
surement of a 21-year-old male patient1 (Mr. P.) with myelogenous leu-
kemia in the course of a receptive therapy session. The patient was
recumbent on a hospital bed, while the therapist was turned to him and
played an Arabian/Turkish lute and a harpsichord. At the time of mea-
surement, Mr. P. received a block of chemotherapy. Prior to measure-
ments he complained of weakness, fatigue, diffuse pain and
indisposition.
1. At the pediatric oncology station of the children and women’s hospital in Linz (Aus-tria).
An example of measurement of a healthy test subject in a traditional “healing dance”
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
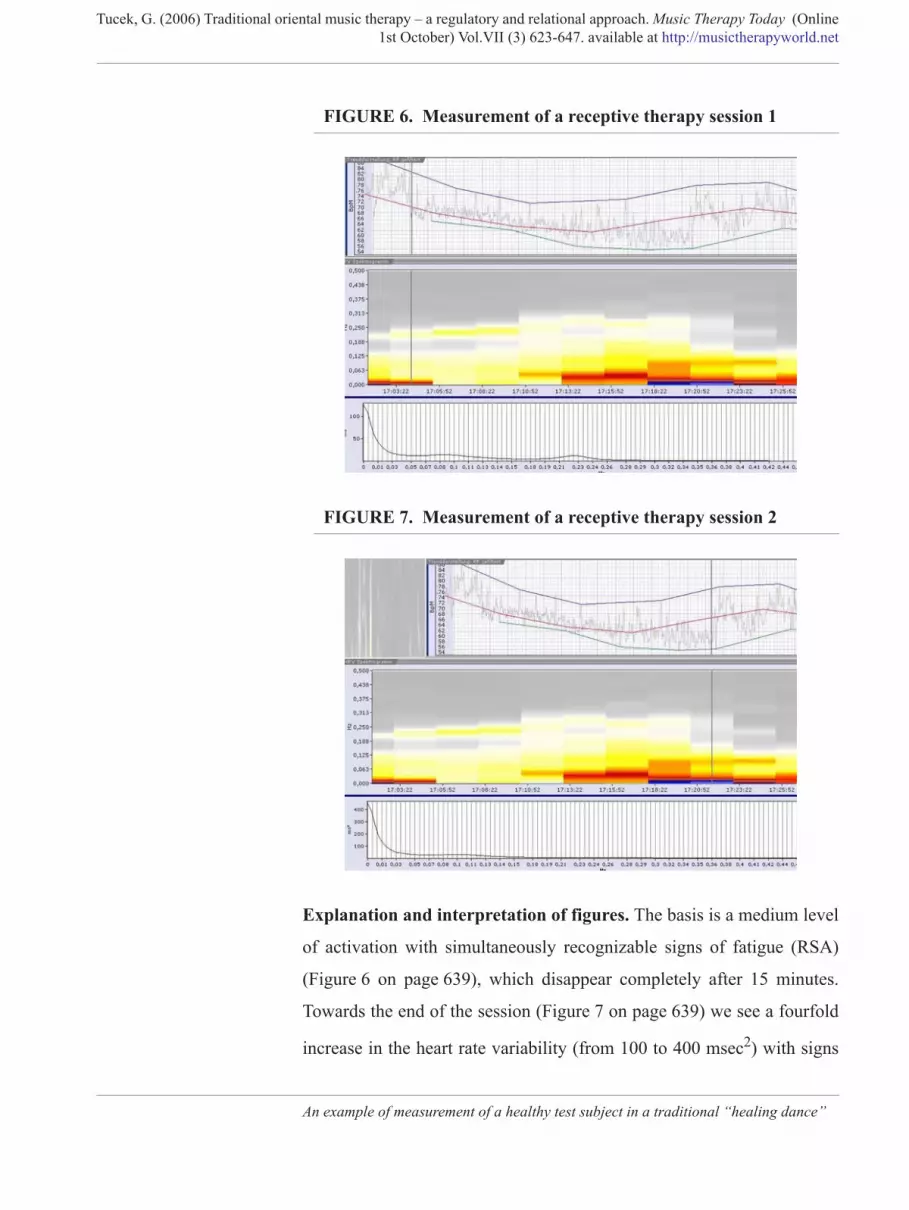
FIGURE 6. Measurement of a receptive therapy session 1
FIGURE 7. Measurement of a receptive therapy session 2
Explanation and interpretation of figures. The basis is a medium level
of activation with simultaneously recognizable signs of fatigue (RSA)
(Figure 6 on page 639), which disappear completely after 15 minutes.
Towards the end of the session (Figure 7 on page 639) we see a fourfold
increase in the heart rate variability (from 100 to 400 msec2) with signs
An example of measurement of a healthy test subject in a traditional “healing dance”
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
of physical activation (blue colouring in the low frequency spectral
range). The patient’s heart rate fell from a mean value of 82 to 58 beats
per minute in the course of the session. This indicates that the reduced
general state described by the patient prior to therapy, i.e. sensations of
weakness, sickness and diffuse pain, was transformed to a vegetative sta-
bilization with reduced pain (heart rate reduction), increased vitality
(HRV increase to the fourfold amount) and disappearance of sickness
(patient’s spontaneous remark after session). This interpretation was also
confirmed in the interview on the patient’s subjective state of health after
the session.
EXAMPLE 2: A SMARD watch – another system of non-invasive measurement and
analysis for regulatory diagnostics - involves measurements of the
parameters heart frequency and pulse frequency (HF and PF), muscular
An example of measurement of a healthy test subject in a traditional “healing dance”
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
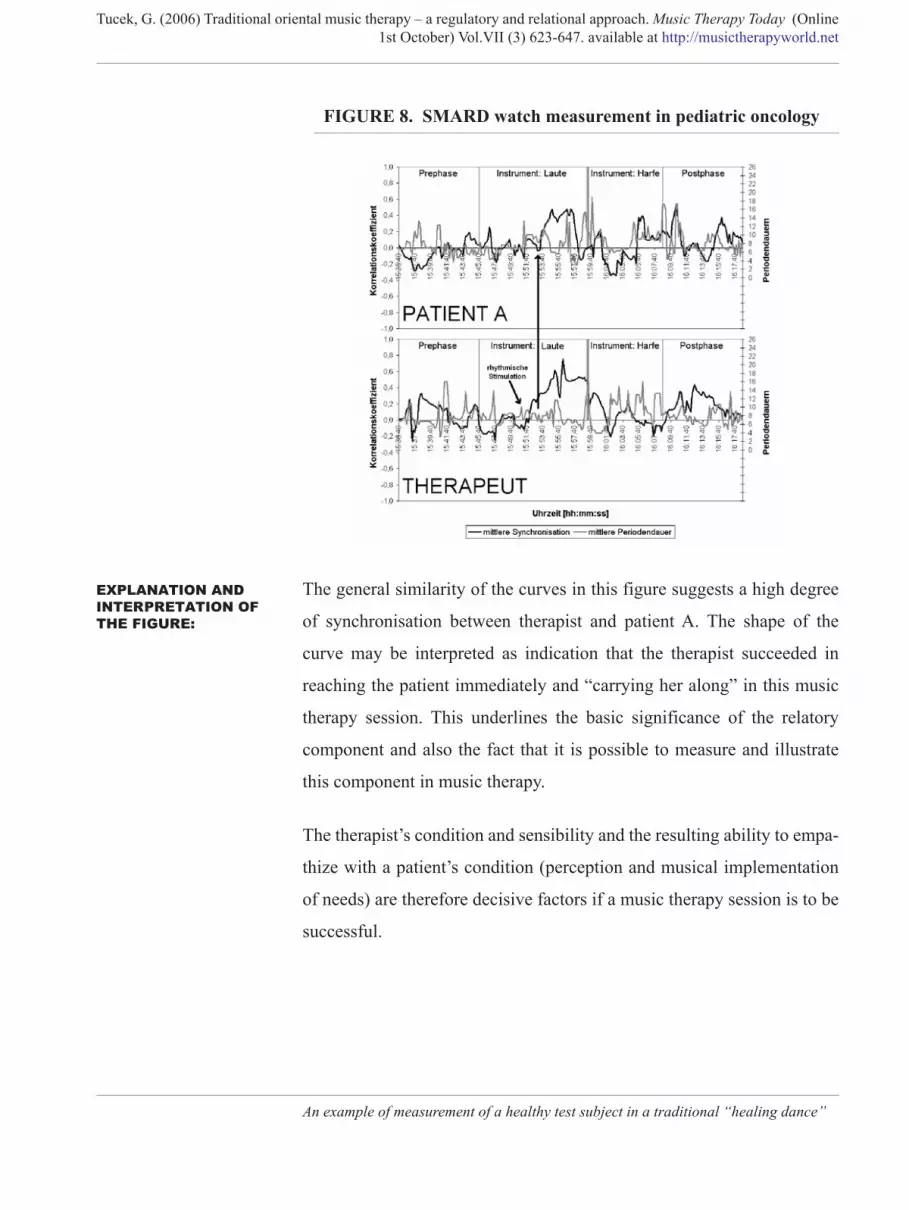
FIGURE 8. SMARD watch measurement in pediatric oncology
EXPLANATION AND INTERPRETATION OF THE FIGURE:
The general similarity of the curves in this figure suggests a high degree
of synchronisation between therapist and patient A. The shape of the
curve may be interpreted as indication that the therapist succeeded in
reaching the patient immediately and “carrying her along” in this music
therapy session. This underlines the basic significance of the relatory
component and also the fact that it is possible to measure and illustrate
this component in music therapy.
The therapist’s condition and sensibility and the resulting ability to empa-
thize with a patient’s condition (perception and musical implementation
of needs) are therefore decisive factors if a music therapy session is to be
successful.
An example of measurement of a healthy test subject in a traditional “healing dance”
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
Summary & outlook:
Experienced music therapy researchers know the difficulties of clinical
practice with regard to replicability and standardization (compare: Tucek,
in Aldridge (ed.), (2005); Scharinger, (2006). But on the other hand there
is a legitimate demand for “hard facts” to verify therapy efficiency. A
general discussion of this subject is beyond the scope of this presentation,
but I would like to underline the two essential advantages of the
approaches described here:
• Both measurement methods allow a music therapist flexibility in his interventions with individual patients without rendering the measuring procedure worthless.
• Both measurement methods produce physiological “hard facts”, e.g. heart and pulse frequency (HF and PF), muscular activity (EMG), skin potential (HP), heart rate variability (HRV) etc.
The measuring methods described here are an additional tool for thera-
pists to reflect patients’ feedback and their own perceptions and observa-
tions of a given situation on the basis of objective measurements. These
approaches open up new possibilities and perspectives for evaluation of
processes in music therapy.
A large number of measured data collected so far confirm the trend found
in the examples presented here. We have now started to study long-term
therapy effects of traditional oriental music therapy by research into
patients’ quality of sleep1.
1. In short: we assume a relation between the quality of an individual’s sleep and his or her regenerative abilities.
Summary & outlook: 642
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
References
Aldridge, David (ed.) Music Therapy and Neurological Rehabilitation
Güvenc, R.O. (1985). Geschichtlicher Abriss der Musiktherapie im
Allgemeinen und im Besonderen bei den Türken. Band 1 der Studi-
entexte der Schule f. Altorientalische Musik - und Kunsttherapie,
Eigenverlag, A-3924 Schloss Rosenau, Niederneustift 66.
References 643
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
Hesse, H.P. (2003). Musik und Emotion. Wissenschaftliche Grundlagen
des Musikerlebens. Wien; Springer Wien New York.
Hildebrandt, G. & Moser, M. & Lehofer, M. (1998). Chronobiologie und
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
Wissenschaften. Vol 6. Institut für Geschichte der Arabisch - Islam-
ischen Wissenschaften an der Johann Wolfgang Goethe Universität
Frankfurt / Main.
Scharinger, E. (2006). Altorientalische Musiktherapie als adjuvante
Therapieform bei Patienten mit Depressiven Episoden. Abschlus-
sarbeit des Studiengangs Altorientalischer Musiktherapie (Jg. 2000
– 2005) am Institut für Ethnomusiktherapie. Schloss Rosenau.
Schipperges H. (1987). Eine "Summa Medicinae" bei Avicenna. Zur
Krankheitslehre und Heilkunde des Ibn Sina (980 - 1037). Springer
Verlag Berlin – Heidelberg.
Shiloah, A. (2002). Die Islamische Musik. In: Welt des Islam. Bernard
Lewis (ed.) Orbis Verlag München.
Tucek, G. (2003a). Altorientalische Musiktherapie im Spannungsfeld
zwischen interkulturellem Dialog und transkultureller Anwendung.
Vom traditionellen Wissenssystem zum transkulturellen Wissen-
stransfer. Dissertation zur Erlangung des Doktorgrades der Philoso-
phie an der Fakultät für Human- und Sozialwissenschaften der
Universität Wien.
Tucek, G. (2003b). Altorientalische Musiktherapie im interkulturellen
Dialog - Kulturimmanente und kulturtranszendente Aspekte im
Menschenbild In: Helga Egner (ed.) Heilung und Heil. Begegnung -
Tucek, G. (2005a). "Traditional Oriental Music Therapy" in neurological
rehabilitation. In: Aldridge, David (ed.) Music Therapy and Neuro-
References 645
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
Tucek, G. et al. 2006: The revival of Traditional Oriental Music Therapy
discussed by cross cultural reflections and a pilot scheme of a quan-
titative EEG-analysis for patients in Minimally Responsive State,
in: Music Therapy Today (Online) Vol.VII (1), (March) 39-64.
available at http://musictherapyworld.net.
INTERNET: www. ArztScout.com (13.7.06).
References 646
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
Author’s details:
FIGURE 9. Gerhard Tucek
Music therapist, specific interests: neurological and cardiological reha-
bilitation, pediatric oncology, work with handicapped persons; clinical
therapy research; practice research. University education: studies of
applied cultural sciences (Mag.phil.) and ethnology (Dr.phil.); university
Author’s details: 647
Tucek, G. (2006) Traditional oriental music therapy – a regulatory and relational approach. Music Therapy Today (Online1st October) Vol.VII (3) 623-647. available at http://musictherapyworld.net
training course in practice research; studies of traditional oriental music
therapy with Dr. Oruc Güvenc
1989 – 2000 establishing the „School for traditional oriental music ther-
apy“ in cooperation with Dr. Oruc Güvenc. Since 1997 Director of the
course in traditional oriental music therapy. Since 2004 Lecturer at the
University for Music and Performing Art, Vienna, since 2005 at the Insti-
tute for Culture & Social Anthropology of Vienna University. Since
2002: Director of the seminar and lecture series „Mensch – Kunst –
Medizin“ (in cooperation with GAMED and Karajan Centrum Vienna).
2004: Founding member and Director of IMARAA (international music
and art research association austria)
ADDRESS: Institute For Ethno-Music-Therapy, Niederneustift 66, A-3924 Schloss
Rosenau (Head of the Institute: Mag. Dr. Gerhard Tucek)
Tel:0043 / 2822 / 51248 Fax +18
e- mail: info(at)ethnomusik.com
THIS ARTICLE CAN BE CITED AS:
Tucek, G. (2006) Traditional oriental music therapy – a regulatory andrelational approach. Music Therapy Today (Online 1st October) Vol.VII(3) 623-647. available at http://musictherapyworld.net